

Good Morning :)
Wishing you all a very happy Sunday & a lucid morning reading experience.
Hyponatremia gets all the attention❗️❗️❗️
Ask any Internist, from resident to HOD, they can go on for hours on hyponatremia.
So I won't discuss that.
Let's focus on HYPERNATREMIA
A 🧵
Wishing you all a very happy Sunday & a lucid morning reading experience.
Hyponatremia gets all the attention❗️❗️❗️
Ask any Internist, from resident to HOD, they can go on for hours on hyponatremia.
So I won't discuss that.
Let's focus on HYPERNATREMIA
A 🧵
Using Fink's Textbook of CCM & Harrison, let's get going.
Hypernatremia, defined as a serum sodium concentration >145 mEq/L, often reflects a relative water deficit rather than a true sodium excess, necessitating a careful assessment of volume status and osmoregulation.
Hypernatremia, defined as a serum sodium concentration >145 mEq/L, often reflects a relative water deficit rather than a true sodium excess, necessitating a careful assessment of volume status and osmoregulation.
Approach to Hypernatremia
1. Confirm Diagnosis
Hypernatremia is S. Sodium >145 mEq/L
Serum & Urine Osmolality:
Compare S. Osmolality with Urine osmolality
⬆️Urine osmolality (>800 mOsm/kg)
Extrarenal causes
⬇️Urine osmolality (<300 mOsm/kg)
Renal losses
1. Confirm Diagnosis
Hypernatremia is S. Sodium >145 mEq/L
Serum & Urine Osmolality:
Compare S. Osmolality with Urine osmolality
⬆️Urine osmolality (>800 mOsm/kg)
Extrarenal causes
⬇️Urine osmolality (<300 mOsm/kg)
Renal losses
2. Assess Volume Status
Hypovolemic:
Evaluate for dehydration (e.g., dry mucous membranes).
Euvolemic:
Consider Diabetes Insipidus or Insensible water losses.
Hypervolemic:
Look for fluid overload due to sodium retention or exogenous sodium administration.
Hypovolemic:
Evaluate for dehydration (e.g., dry mucous membranes).
Euvolemic:
Consider Diabetes Insipidus or Insensible water losses.
Hypervolemic:
Look for fluid overload due to sodium retention or exogenous sodium administration.
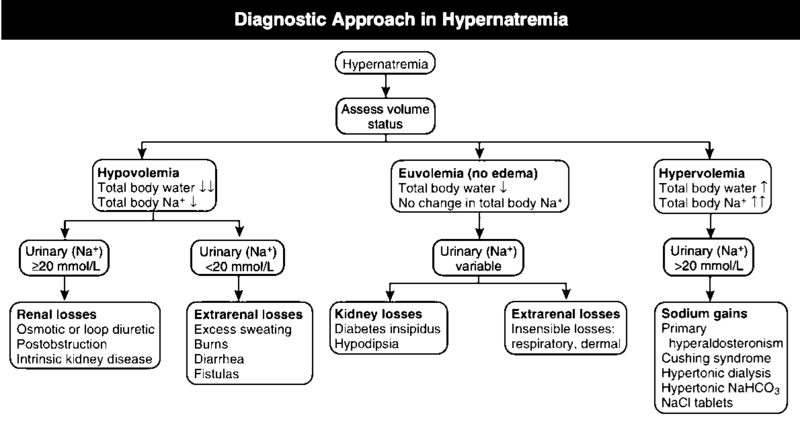
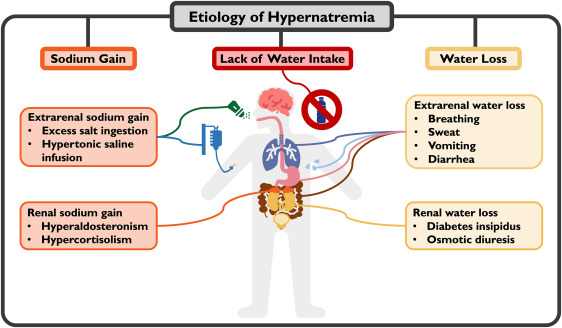
3. Determine Underlying Cause
Renal losses:
Evaluate for DI (central/Nephrogenic), Osmotic Diuresis.
Extrarenal losses:
Assess for diarrhea, vomiting, or excessive sweating.
Iatrogenic causes:
Review medications, for hypertonic saline, diuretics, and soda-bicarb.
Renal losses:
Evaluate for DI (central/Nephrogenic), Osmotic Diuresis.
Extrarenal losses:
Assess for diarrhea, vomiting, or excessive sweating.
Iatrogenic causes:
Review medications, for hypertonic saline, diuretics, and soda-bicarb.
4. Fluid Mx
Correct Volume Deficit:
In ⬇️volemic ⬆️natremia, start 0.9% NaCl until pt. is euvolemic.
Correct Free Water Deficit:
Use (D5W) or 0.45% NS.
In chronic ⬆️natremia (>48 hr), target a ⬇️by 0.5 mEq/L/hr.
In acute ⬆️natremia (<48 hr), target a ⬇️1-2 mEq/L/hr.
Correct Volume Deficit:
In ⬇️volemic ⬆️natremia, start 0.9% NaCl until pt. is euvolemic.
Correct Free Water Deficit:
Use (D5W) or 0.45% NS.
In chronic ⬆️natremia (>48 hr), target a ⬇️by 0.5 mEq/L/hr.
In acute ⬆️natremia (<48 hr), target a ⬇️1-2 mEq/L/hr.
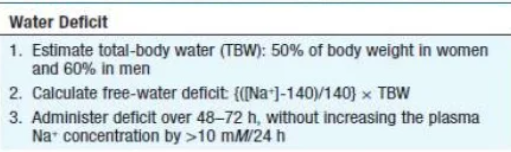
5. Calculate the free water deficit:
Free Water Deficit (FWD) = TBW x (serum [Na] -140) /140
Total Body Water (TBW) is estimated as 0.6 x body weight in males and 0.5 x body weight in females.
Administer fluids to correct the calculated deficit gradually over 48–72 hours.
Free Water Deficit (FWD) = TBW x (serum [Na] -140) /140
Total Body Water (TBW) is estimated as 0.6 x body weight in males and 0.5 x body weight in females.
Administer fluids to correct the calculated deficit gradually over 48–72 hours.
6. Address Underlying Disease:
In Central DI, administer Desmopressin (DDAVP).
In Nephrogenic DI, use thiazide diuretics or amiloride to reduce polyuria.
Adjust treatment based on iatrogenic causes, STOP contributing agents (e.g., diuretics or hypertonic solutions).
In Central DI, administer Desmopressin (DDAVP).
In Nephrogenic DI, use thiazide diuretics or amiloride to reduce polyuria.
Adjust treatment based on iatrogenic causes, STOP contributing agents (e.g., diuretics or hypertonic solutions).
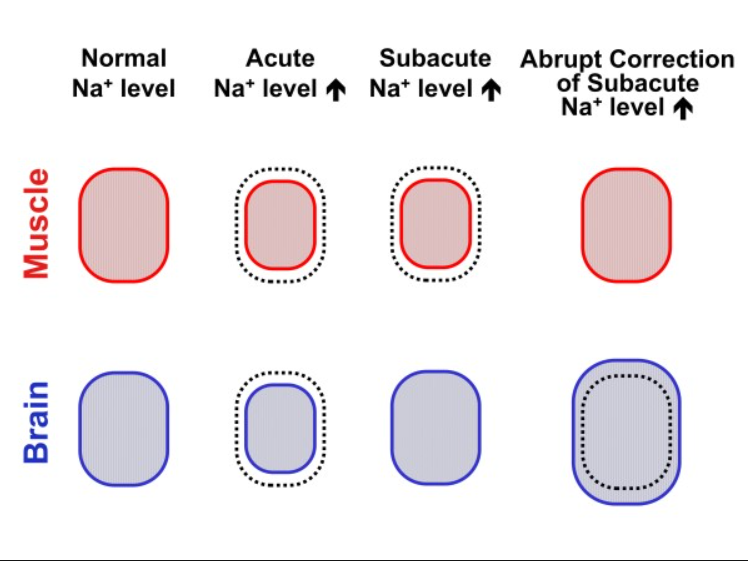
7. Avoid Rapid Correction
Aim for slow correction in chronic hypernatremia to avoid osmotic demyelination syndrome (ODS).
Stop or slow down sodium correction if neurological signs of cerebral edema (e.g., altered mental status) appear.
Aim for slow correction in chronic hypernatremia to avoid osmotic demyelination syndrome (ODS).
Stop or slow down sodium correction if neurological signs of cerebral edema (e.g., altered mental status) appear.
8. Pharmacologic Adjuncts(if necessary):
For Central DI, administer DDAVP intranasally, S/C, or I/V.
For Nephrogenic DI, use amiloride, thiazide diuretics, and, dietary sodium restriction.
Loop diuretics may be used in cases of ⬆️volemic ⬆️natremia to promote Na+ excretion.
For Central DI, administer DDAVP intranasally, S/C, or I/V.
For Nephrogenic DI, use amiloride, thiazide diuretics, and, dietary sodium restriction.
Loop diuretics may be used in cases of ⬆️volemic ⬆️natremia to promote Na+ excretion.

Needless to say, at every stage it requires due diligence.
I will try to explain the detailed pathophysiology, mechanism of action in subsequent threads.
And yes, there's nothing new here. I'm writing notes, not textbook. :)
Hopefully, one day, maybe a textbook, too.😁
I will try to explain the detailed pathophysiology, mechanism of action in subsequent threads.
And yes, there's nothing new here. I'm writing notes, not textbook. :)
Hopefully, one day, maybe a textbook, too.😁
Feel free to share the content. Follow
@kamdar_j
Tag more #MedED #FOAMed #MedTwitter #MedX accounts.
@nihardesai7
@critconcepts
@NicoGagelmann
@AvrahamCooperMD
@drkeithsiau
@ClementLeeMD
@TheIntensivist_
@PulmCrit
@CuriousClinPod
@Crit_Care
@CriticalCareNow
@IM_Crit_
@CritCareNotes
@drmohansai
@kamdar_j
Tag more #MedED #FOAMed #MedTwitter #MedX accounts.
@nihardesai7
@critconcepts
@NicoGagelmann
@AvrahamCooperMD
@drkeithsiau
@ClementLeeMD
@TheIntensivist_
@PulmCrit
@CuriousClinPod
@Crit_Care
@CriticalCareNow
@IM_Crit_
@CritCareNotes
@drmohansai
جاري تحميل الاقتراحات...