

Idiopathic intracranial hypertension (IIH)
This relatively common disorder is an important secondary cause of headache and can cause permanent vision loss. Let’s dive into the presentation, work up, and diagnosis together!
#neurology #FOAMed #MedEd #neurotwitter #tweetorial
This relatively common disorder is an important secondary cause of headache and can cause permanent vision loss. Let’s dive into the presentation, work up, and diagnosis together!
#neurology #FOAMed #MedEd #neurotwitter #tweetorial
IIH is a syndrome characterized by CSF hypertension which is not due to obstruction or other mass-occupying lesion.
The prevalence is about 1 in 100,000 in the general population, but it’s 20 times more common in the highest risk population, obese women < 45.
The prevalence is about 1 in 100,000 in the general population, but it’s 20 times more common in the highest risk population, obese women < 45.
The cause is not known, but one theory involves a positive feedback loop of disordered CSF production in response to intracranial hypertension.

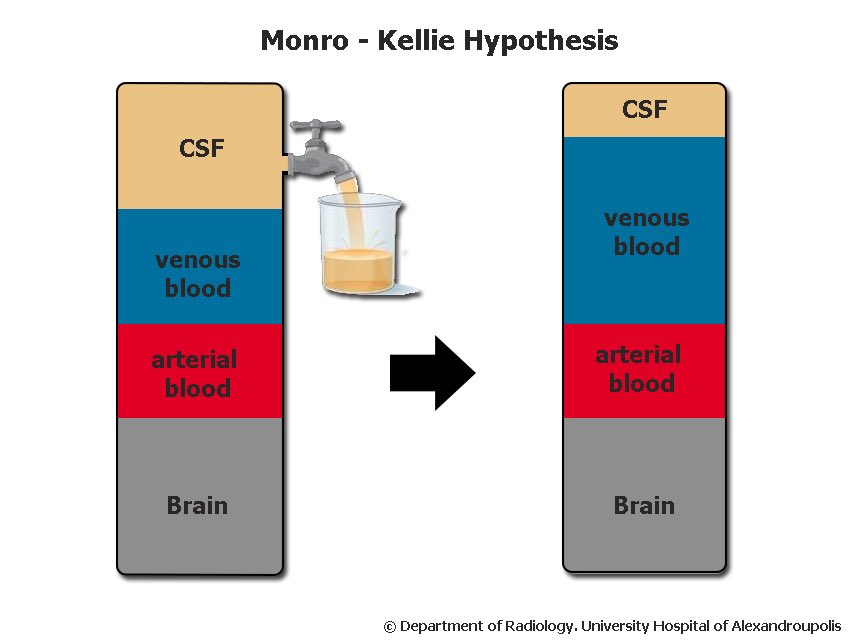
The Monro-Kellie doctrine helps us understand intracranial hypertension.
In a homeostatic state, the intracranial compartment is an “iron quadrangle” of CSF, venous and arterial blood, and brain tissue. A change in one compartment will affect the others.
In a homeostatic state, the intracranial compartment is an “iron quadrangle” of CSF, venous and arterial blood, and brain tissue. A change in one compartment will affect the others.
Risk factors for IIH include:
- female sex
- age 15-44
- obesity
- sleep apnea
- certain meds (eg vitamin A analogs, tetracyclines)
- venous sinus stenosis (primary or secondary)
- female sex
- age 15-44
- obesity
- sleep apnea
- certain meds (eg vitamin A analogs, tetracyclines)
- venous sinus stenosis (primary or secondary)
Symptoms:
- Headache (esp “reverse orthostatic” HA worse when laying down or in the morning)
- Pulsatile tinnitus
- Visual symptoms
> Transient visual obscurations
(particularly w/ Valsalva)
> Photopsia
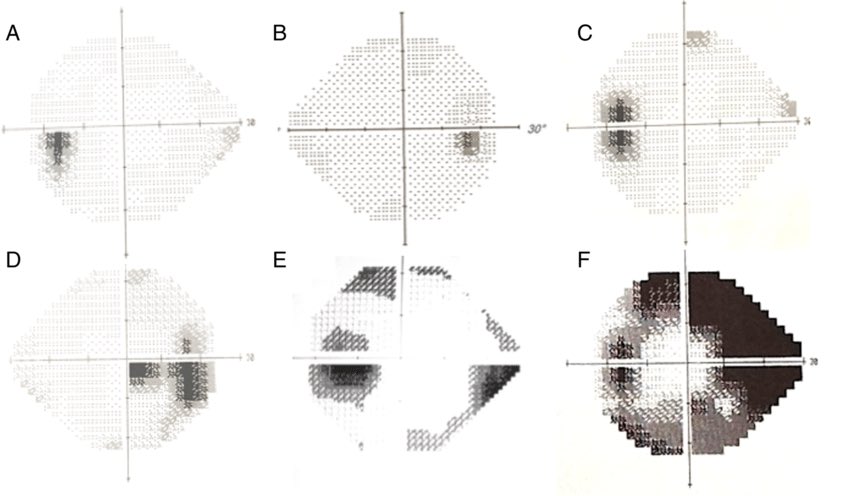
> Visual field constriction
- Headache (esp “reverse orthostatic” HA worse when laying down or in the morning)
- Pulsatile tinnitus
- Visual symptoms
> Transient visual obscurations
(particularly w/ Valsalva)
> Photopsia
> Visual field constriction
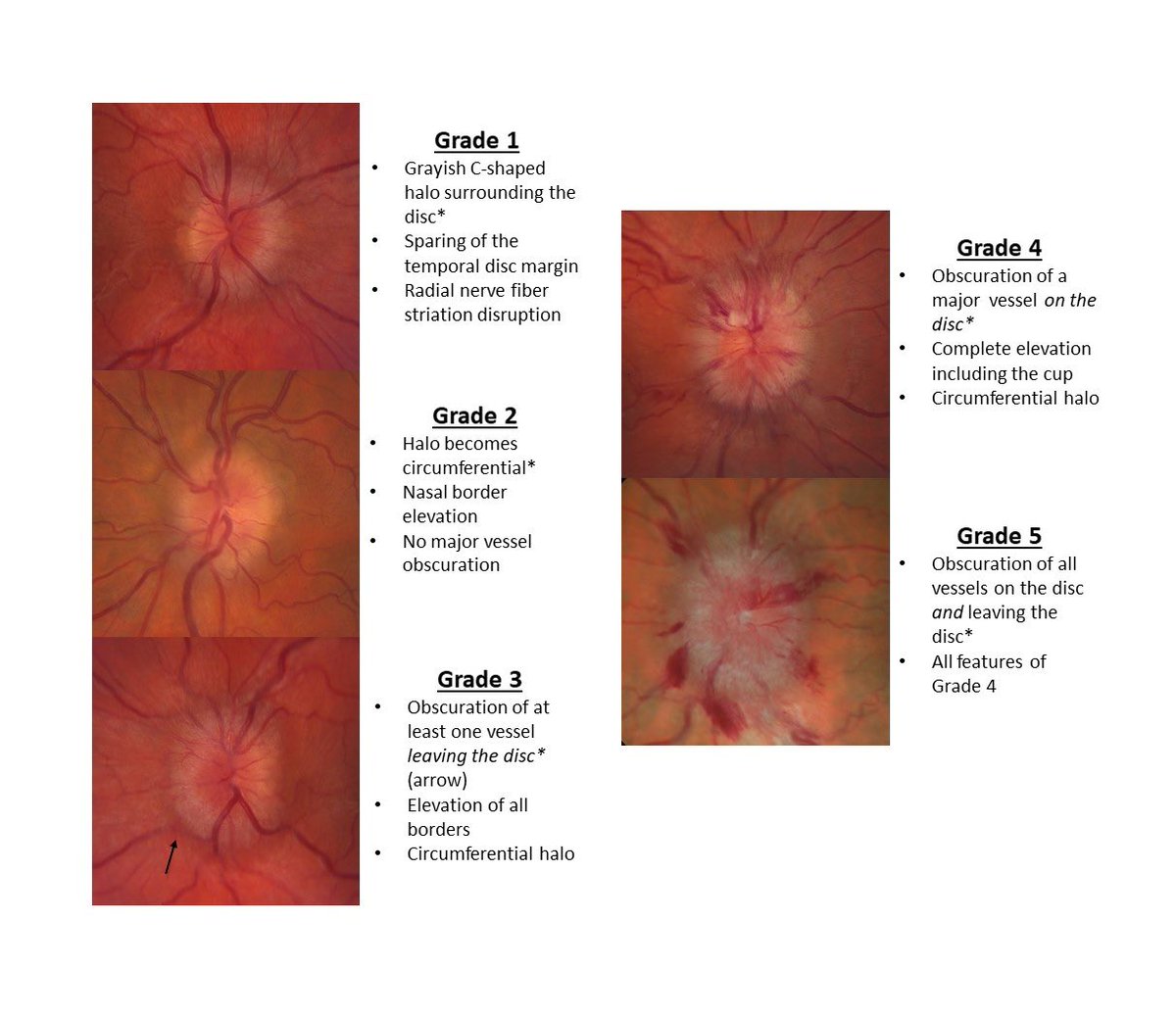
Exam should be essentially normal with the exception of two findings:
- Papilledema on fundoscopy
- Unilateral or bilateral CN 6 palsy (commonly damaged in intracranial hypertension of any kind)
- Papilledema on fundoscopy
- Unilateral or bilateral CN 6 palsy (commonly damaged in intracranial hypertension of any kind)
Diagnosis is based on the modified Dandy criteria, essentially requiring:
- Signs and symptoms of IIH
- No mass occupying lesion or other 1:1 cause of intracranial hypertension
- Elevated CSF opening pressure
- Signs and symptoms of IIH
- No mass occupying lesion or other 1:1 cause of intracranial hypertension
- Elevated CSF opening pressure
Work up will require:
- MRI imaging to exclude tumor, venous sinus thrombus, and other structural causes of intracranial hypertension
- LP with opening pressure to demonstrate CSF hypertension and exclude meningitis or CNS inflammation
- MRI imaging to exclude tumor, venous sinus thrombus, and other structural causes of intracranial hypertension
- LP with opening pressure to demonstrate CSF hypertension and exclude meningitis or CNS inflammation
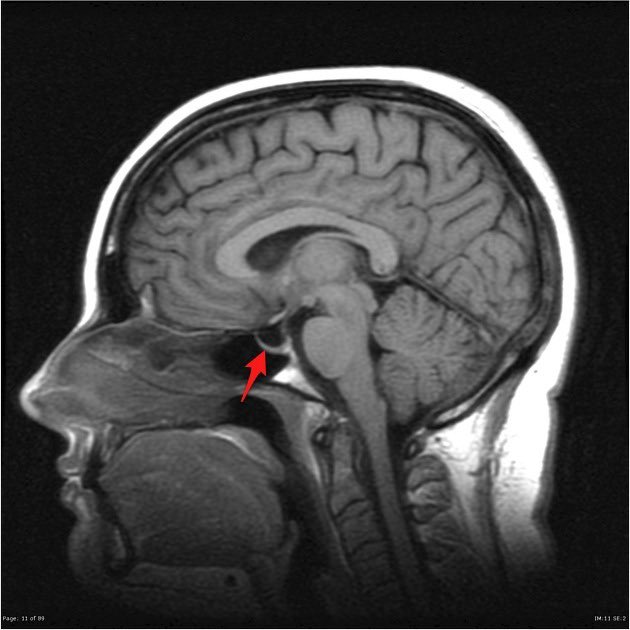
Common radiographic findings of IIH include:
- Partially empty sella
- Optic disc bulging
- Posterior globe flattening
- Tortuosity of optic nerve
- Optic nerve sheath edema
- Transverse sinus stenosis
- Partially empty sella
- Optic disc bulging
- Posterior globe flattening
- Tortuosity of optic nerve
- Optic nerve sheath edema
- Transverse sinus stenosis


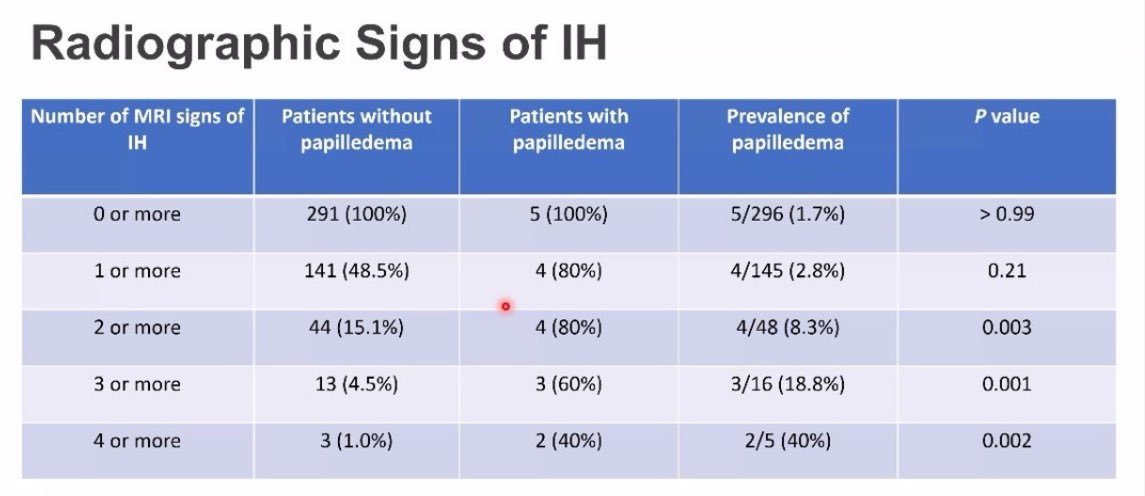
It’s important to note that all of these findings are nonspecific. Look for a cluster of findings with symptoms.
In a sequential MRI series, a single radiographic finding had a >95% chance of being incidental. If your patient is asymptomatic, the +LR is even lower.
In a sequential MRI series, a single radiographic finding had a >95% chance of being incidental. If your patient is asymptomatic, the +LR is even lower.
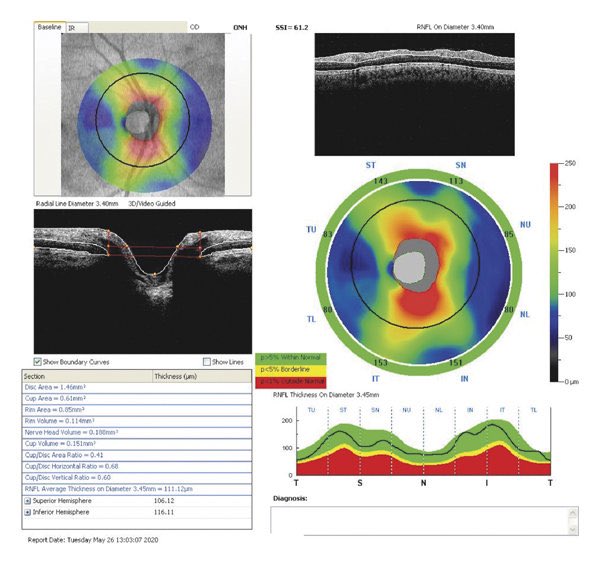
Patients should also follow with ophthalmology or neuro-ophthalmology for formal visual field testing and potentially more advanced testing like nerve fiber layer thickness monitoring with OCT. Ongoing monitoring is useful to assess treatment efficacy.
TREATMENT
The feared outcome of IIH is vision loss, so treatment revolves around preventing this. Treatment of other symptoms like headache and tinnitus are important but secondary goals.
The feared outcome of IIH is vision loss, so treatment revolves around preventing this. Treatment of other symptoms like headache and tinnitus are important but secondary goals.
Addressing risk factors such as untreated sleep apnea, weight loss in the case of obesity, and cessation of offending meds should be our very first step.
First line medical treatment is with carbonic anhydrase inhibitors. This generally means acetazolamide, although topiramate has emerged as a potentially equally effective treatment which additionally helpful in treating headaches.
Second-line options include loop diuretics.
Second-line options include loop diuretics.
Surgery is generally reserved for refractory cases or for those with advanced or rapidly progressive vision loss.
There are four surgical options: optic nerve sheath fenestration, CSF diversion (shunting), venous sinus stenting, and bariatric surgery.
There are four surgical options: optic nerve sheath fenestration, CSF diversion (shunting), venous sinus stenting, and bariatric surgery.
None of these surgeries have been studied head-to-head, so comparisons are limited to large case series.
The choice of surgery will depend on the presence of treatable pathology (transverse sinus stenosis, severe obesity) as well as availability.
The choice of surgery will depend on the presence of treatable pathology (transverse sinus stenosis, severe obesity) as well as availability.
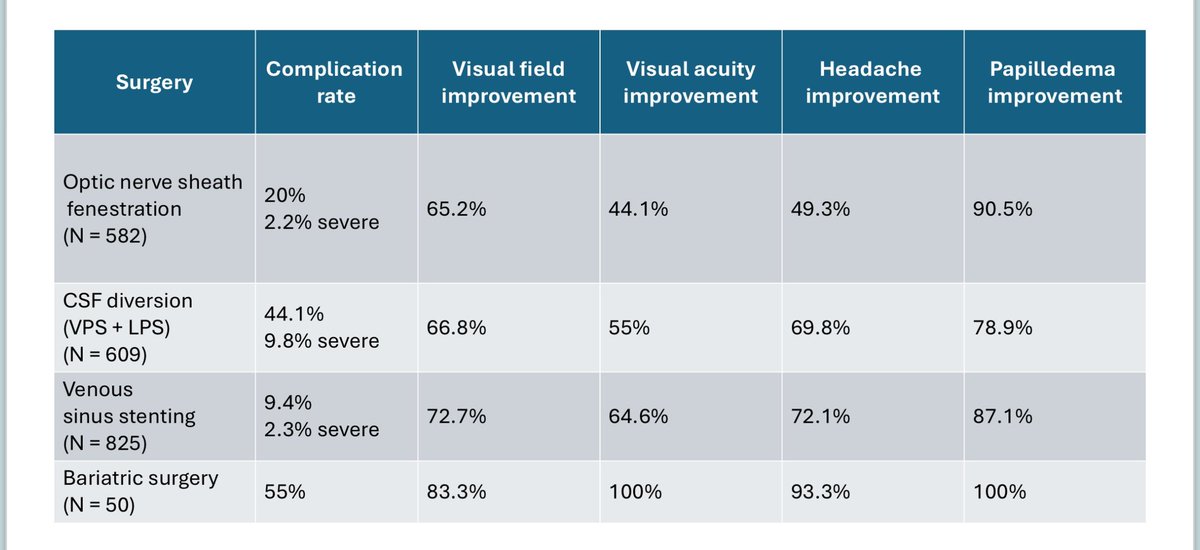
CSF shunting has fallen out of favor recently, having a much higher complication rate and equivalent efficacy. Venous sinus stenosis is emerging as a more popular surgical approach and has similar quality of supportive data as the other surgical treatments.
Take-home points:
- IIH is relatively common and requires MRI and LP to diagnose
- Incidental IIH-like findings are very common; look for symptoms and multiple findings
- First line treatment is with risk factor management and acetazolamide
- Ongoing monitoring is crucial
- IIH is relatively common and requires MRI and LP to diagnose
- Incidental IIH-like findings are very common; look for symptoms and multiple findings
- First line treatment is with risk factor management and acetazolamide
- Ongoing monitoring is crucial
جاري تحميل الاقتراحات...