

ICU Pharmacology Secrets:
This is another random collection of pharmacology pearls that I witnessed & wrote down during the last two months.
And so it begins:
1. Hydralazine (H) is a widely used arterial vasodilator; especially in 🇺🇸, it is mostly used to treat
This is another random collection of pharmacology pearls that I witnessed & wrote down during the last two months.
And so it begins:
1. Hydralazine (H) is a widely used arterial vasodilator; especially in 🇺🇸, it is mostly used to treat
asymptomatic hypertension in the hospital setting. Has anybody seen the order: “Hydralazine 10 mg iv PRN for SBP > 180”? Medtwitter is full of posts deriding H use, but this practice does not go away & sometimes it even becomes part of the outpatient treatment regimen; probably
a remnant of the V-HeFT I study? A much less known fact is that H is linked to the development of drug-induced anti-neutrophil cytoplasmic antibody-associated vasculitis & drug-induced lupus. These require not just discontinuation of H but immunosuppression too. Be aware! 😬
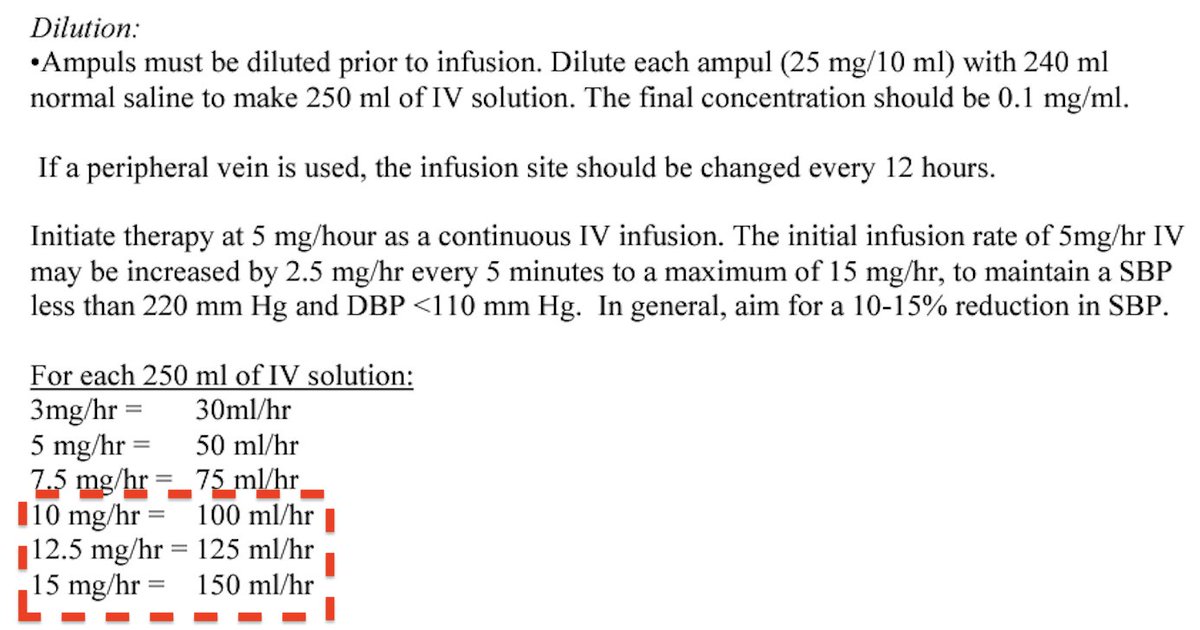
2. Nicardipine (N) is another widely used Ca-channel blocker working as arterial vasodilator & administered as iv infusion usually in pts w hypertensive emergency. The recommended starting dose is 5 mg/h, w titration in ⬆️ of 2.5 mg/h to a max 15 mg/h every 5-15 min. But, you can
bolus 2.5 mg iv for more rapid BP control (you didn’t hear this from me…). Fun fact: many times, N is diluted in large volumes of normal saline. So, if u need 15 mg/h, u end up infusing 3 l of NS/day! It does not sound ideal in a pt w pulm edema due to HTN emergency, does it? 😳
3. Esmolol (E) is a rapid-onset iv cardioselective β-1 blocker used in managing supraventricular tachycardia/atrial fibrillation-flutter/periop-postop hypertension. Its half-life is 9 min & it is metabolized by erythrocyte esterases. The recommended bolus dose is 500-1000 mcg/kg
over 30 sec, followed by titration to a maximum dose of 300 mcg/kg/min.
Personal bias #1: I never understood why E is dosed in mcg/kg/min while diltiazem, for example, is dosed in mg/min!
Personal bias #2: IMHO, giving > 500 mcg/kg bolus can be problematic &
Personal bias #1: I never understood why E is dosed in mcg/kg/min while diltiazem, for example, is dosed in mg/min!
Personal bias #2: IMHO, giving > 500 mcg/kg bolus can be problematic &
going over 200 mcg/kg/min will rarely enhance its antihypertensive effect.
Fun fact #1: similar to nicardipine, E is usually diluted in large volumes. So, if you need 300 mcg/kg/min for an 80 kg person, you will infuse 150 ml/h!
Fun fact #1: similar to nicardipine, E is usually diluted in large volumes. So, if you need 300 mcg/kg/min for an 80 kg person, you will infuse 150 ml/h!

Fun fact #2: When a pt on E infusion becomes hypoglycemic, there will be no tachycardia, therefore diabetic pts on esmolol should be closely monitored.
Fun fact #3: E is metabolized to methanol, so if it is administered in large doses for a prolonged time,
Fun fact #3: E is metabolized to methanol, so if it is administered in large doses for a prolonged time,
methanol toxicity should be suspected, especially if the pt develops an otherwise unexplained high anion gap/osmolar gap metabolic acidosis... 🤯
4. Although it happens rarely (probably <0.5%), the administration of thrombolytics is associated w anaphylaxis. If you work in a busy ED/ICU, please remember that a crashing pt post t-PA infusion may not have cerebral hemorrhage or refractory RV failure but anaphylactic shock 😨
5. Myoclonus is a very frequent side-effect of etomidate (E) administration, complicating 50-80% of cases. The only reason we don’t see it often in the ICU is that we perform RSI & follow E with a paralytic. But, if you start using etomidate alone,
for example to sedate a patient in rapid atrial fibrillation prior to electrical cardioversion, you will see it frequently. Personal bias: I use ketamine for intubation... 😊
6. Cefepime (C) is a 4th-generation cephalosporin that I witness being used very often in the ED or the wards (as part of the cefepime-vancomycin cocktail) when a septic patient has “penicillin allergy” listed in the chart. This is fine but it is frequently forgotten that
C has no activity against anaerobic pathogens. Therefore, even though now we know that aspiration pneumonia does not seem to need anaerobic coverage, the truth is that in cases of intra-abdominal infections (eg, perforated diverticulitis), C is clearly inadequate treatment.
Fun fact: vancomycin is active against many anaerobic gram-positive bacilli & cocci, including Bacillus spp., Actinomyces spp., Clostridium spp., Corynebacterium spp, Peptostreptococcus etc... 🤷♂️
7. Not every cirrhotic patient with ascites needs to be on scheduled albumin around the clock from the day of admission until the day of discharge. Similarly, not every patient on furosemide or bumetanide drip requires albumin! Enough said… 🤬
8. In cases of unexplained hyperkalemia in hospitalized pts, please do not overlook the role of heparin (H). H can inhibit aldosterone synthesis even at low doses & lead to ⬆️ Na excretion & ⬆️ K retention. This is more pronounced in elderly pts w renal dysfunction & diabetes 🧐
9. Speaking about unexplained electrolyte abnormalities: If you manage end-stage renal disease pts w difficult to control hyperphosphatemia, please take a look at their medications list. Many of them can contribute substantial amounts of inorganic phosphate to a pt’s daily phos
burden, and this varies significantly among manufacturers. If a patient receives just 4 drugs - amlodipine, lisinopril, omeprazole, diclofenac - the added burden is almost 800 mg of phosphate/day, very close to the recommended daily phosphate intake for dialysis patients 🤫

10. Clozapine is an FDA-approved atypical antipsychotic for treatment-resistant schizophrenia. It has a number of esoteric but quite real side effects such as agranulocytosis, metabolic syndrome, myocarditis, seizures etc. If it is discontinued for >2 days, (eg, in a pt w ileus),
the “2-days rule” should be followed & the drug should be restarted at a lower dose to reduce the risk of bradycardia, hypotension & syncope. Of course, over the years I have seen cases where the drug was restarted by the medical provider at full dose & nothing bad happened! But,
at some point ignorance will come back to bite us! 🙄
Thanks for following along! Feel free to correct me & share your experiences.
Thanks for following along! Feel free to correct me & share your experiences.
Some useful references:
kidney-international.org
dartmouth-hitchcock.org
shpa.org.au
ahajournals.org
frontiersin.org
ncbi.nlm.nih.gov
shmpublications.onlinelibrary.wiley.com
bmj.com
ncbi.nlm.nih.gov
ncbi.nlm.nih.gov
kidney-international.org
dartmouth-hitchcock.org
shpa.org.au
ahajournals.org
frontiersin.org
ncbi.nlm.nih.gov
shmpublications.onlinelibrary.wiley.com
bmj.com
ncbi.nlm.nih.gov
ncbi.nlm.nih.gov
ahajournals.org/doi/10.1161/ST…
Association Between Intravenous Thrombolysis and Anaphylaxis Among Medicare Beneficiaries With Acute Ischemic Stroke
Background and Purpose— Allergic reactions, including anaphylaxis, can sometimes occur after intrave...
dartmouth-hitchcock.org/sites/default/…

bmj.com/rapid-response…
Do not forget heparin induced hyperkalemia.
ncbi.nlm.nih.gov/pmc/articles/P…
Phosphates in medications: Impact on dialysis patients
Maintaining phosphorus balance in in-center hemodialysis (ICHD) patients is problematic despite reco...

frontiersin.org/articles/10.33…
Comparison of the Effectiveness of Various Drug Interventions to Prevent Etomidate-Induced Myoclonus: A Bayesian Network Meta-Analysis
BackgroundMyoclonic movement is a very common but undesirable phenomenon during the induction of gen...

ncbi.nlm.nih.gov/books/NBK54223…
Cefepime
Cefepime is a cephalosporin in the beta-lactam class of antibiotics used to manage and treat gram-ne...

kidney-international.org/article/S0085-…
Anti-neutrophil cytoplasmic antibody associated glomerulonephritis complicating treatment with hydralazine
Hydralazine, a widely used therapy for hypertension and heart failure, can elicit autoimmune disease...
ncbi.nlm.nih.gov/pmc/articles/P…
Clozapine is the approved option in treatment-resistant schizophrenia and requires careful management
Clozapine is the only agent approved for treatment-resistant schizophrenia, but is underprescribed....

…mpublications.onlinelibrary.wiley.com/doi/10.1002/jh…
Things We Do for No Reason™: Furosemide‐albumin coadministration for diuretic resistance
Click on the article title to read more.
shpa.org.au/publicassets/4…
جاري تحميل الاقتراحات...