

PREVENTING UNDETECTED OESOPHAGEAL INTUBATION. A thread @RCoANews @dasairway @ICS_updates @FICMNews @CollegeODP @SaferSurgeryUK @BACCNUK @MartinBromiley
It is rare
It is fatal
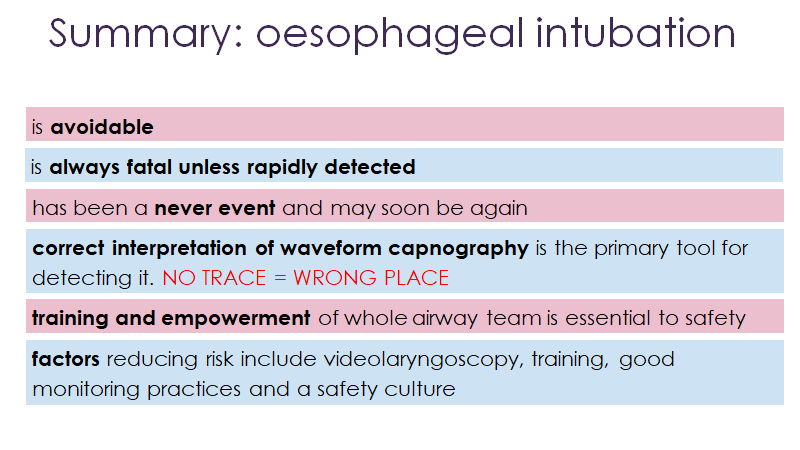
It is avoidable
Sadly it still happens
1/16
rcoa.ac.uk
It is rare
It is fatal
It is avoidable
Sadly it still happens
1/16
rcoa.ac.uk


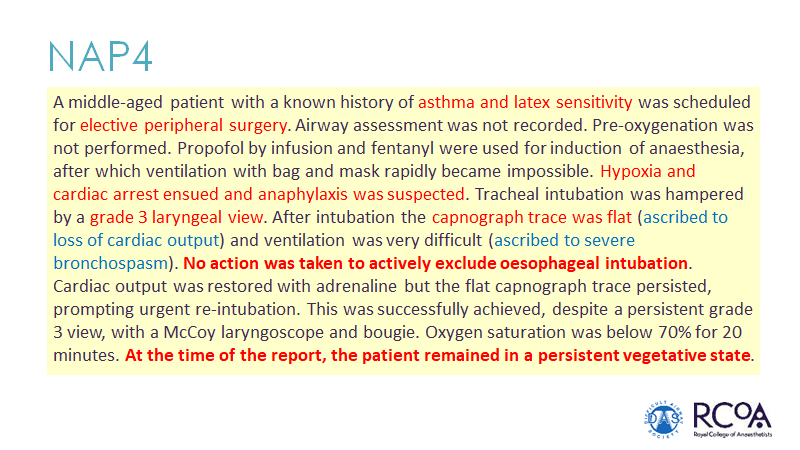
Ten years ago in NAP4 there were 9 cases of undetected oesophageal intubation with harm reported.
No location was exempt.
3/16
No location was exempt.
3/16

Technology - capnography - identifies when intubation fails
It should be used for all tracheal intubations (& remain until after extubation) wherever/whenever they occur
A flat capnograph should be assumed to be due to oesophageal intubation until actively excluded
4/16
It should be used for all tracheal intubations (& remain until after extubation) wherever/whenever they occur
A flat capnograph should be assumed to be due to oesophageal intubation until actively excluded
4/16

Capnography is not an added extra it is a mandatory part and parcel of tracheal intubation.
Standards say so - and have done for years.
associationofanaesthetists-publications.onlinelibrary.wiley.com
5/16
Standards say so - and have done for years.
associationofanaesthetists-publications.onlinelibrary.wiley.com
5/16
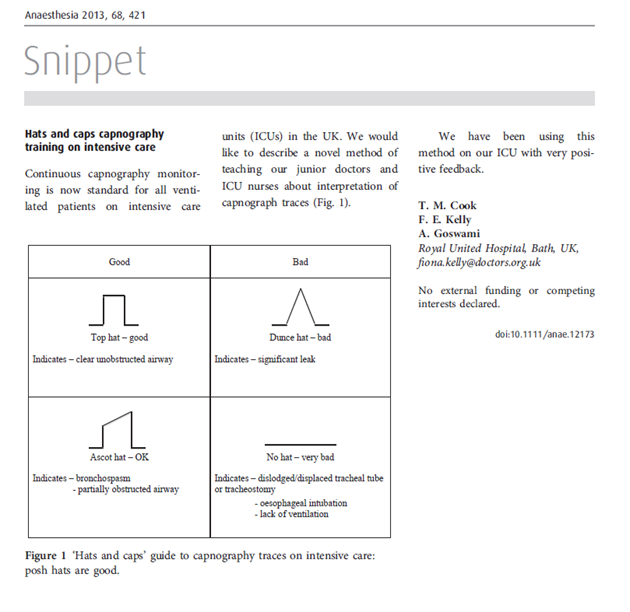
...everyone involved in airway management should be able to interpret a capnograph trace
No its not complex.
Keep it simple.
In Bath we use hats and caps: posh hats are good!
associationofanaesthetists-publications.onlinelibrary.wiley.com
6/16
No its not complex.
Keep it simple.
In Bath we use hats and caps: posh hats are good!
associationofanaesthetists-publications.onlinelibrary.wiley.com
6/16
Yes there are many other cases of a flat capnograph...but it's not anaphylaxis or bronchospasm until you've first excluded oesophageal intubation
The consequences are catastrophic
7/16
The consequences are catastrophic
7/16
This is also the case during cardiac arrest
During cardiac arrest
-a flat capnograph must first be assumed to be due to oesophageal intubation....until this is excluded
-if the tube is in the trachea there will be an attenuated capnograph trace
8/16
During cardiac arrest
-a flat capnograph must first be assumed to be due to oesophageal intubation....until this is excluded
-if the tube is in the trachea there will be an attenuated capnograph trace
8/16


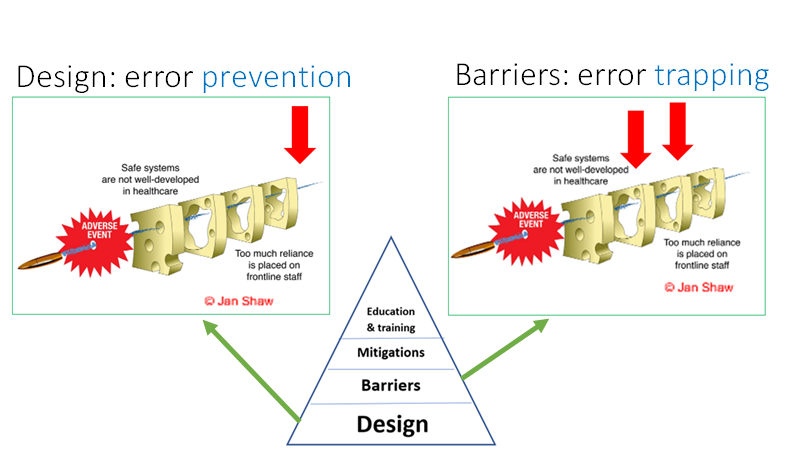
.....but its about more than capnography.
This 'traps' the error but can we prevent the error?
Human factors/ergonomics teaches us that 90% of the solution should be design (prevention) rather than barriers (error trapping)
@Fionafionakel @RCoANews
10/16
This 'traps' the error but can we prevent the error?
Human factors/ergonomics teaches us that 90% of the solution should be design (prevention) rather than barriers (error trapping)
@Fionafionakel @RCoANews
10/16
Some thoughts on error prevention & undetected oesophageal intubation
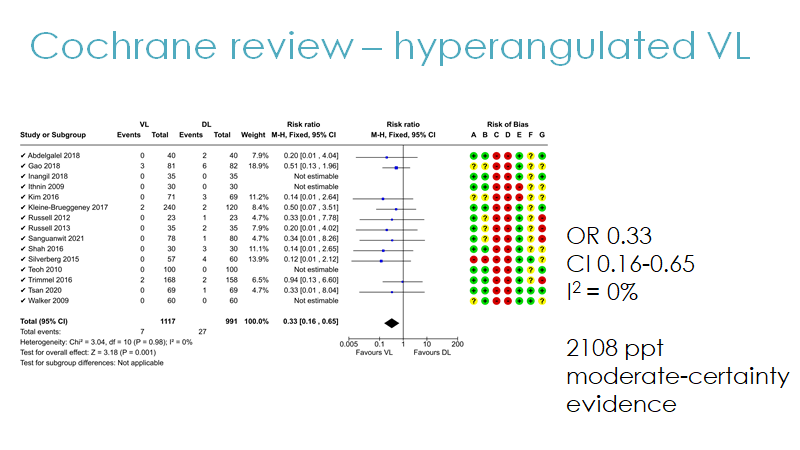
Videolaryngoscopy
Consistent monitoring
Hardware is important in performance (& IS part of human factors and ergonomics)
@Fionafionakel states 'good technical skills make space for good human factors'
11/16
Videolaryngoscopy
Consistent monitoring
Hardware is important in performance (& IS part of human factors and ergonomics)
@Fionafionakel states 'good technical skills make space for good human factors'
11/16

...but training, including & respecting the team changes the culture.
It empowers staff in a crisis.
It's more about behaviour than kit.
'Change intubation from 'me to we'
When I talk about the 'shared airway' I mean everyone on the room can contribute
12/16
It empowers staff in a crisis.
It's more about behaviour than kit.
'Change intubation from 'me to we'
When I talk about the 'shared airway' I mean everyone on the room can contribute
12/16
If coming into a crisis situation - what do you do?
How to apprise the situation & use fresh eyes?
I like SNAPPI
pubmed.ncbi.nlm.nih.gov
13/16
How to apprise the situation & use fresh eyes?
I like SNAPPI
pubmed.ncbi.nlm.nih.gov
13/16

In a crisis behaviour may/will deteriorate.
Even in good people!
Perseveration is common
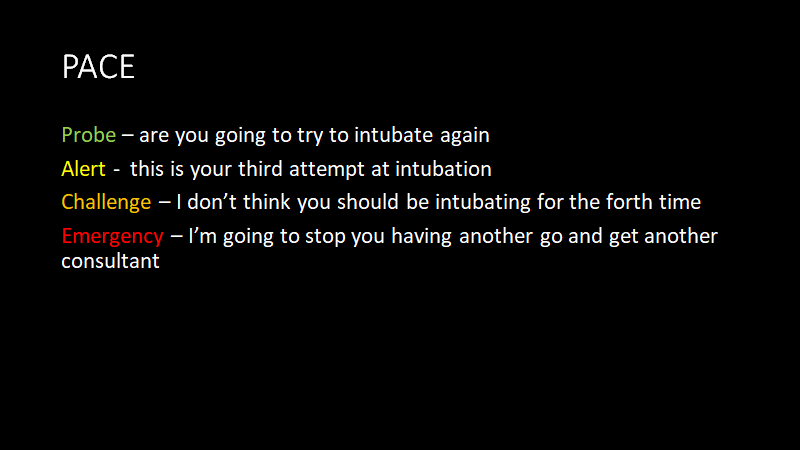
How to intervene safely and professionally
Here I like PACE
14/16
Even in good people!
Perseveration is common
How to intervene safely and professionally
Here I like PACE
14/16
We all need to act together to recognise that we can fail individually & are more likely to succeed as a team.
We need to embrace technology & optimise team behaviour
Lets get rid of undetected oesophageal intubation and avoidable patient harm & deaths.
15/16
We need to embrace technology & optimise team behaviour
Lets get rid of undetected oesophageal intubation and avoidable patient harm & deaths.
15/16
Preventing undetected oesophageal intubation
Let's act.
16/16
Let's act.
16/16

17/16
As an addendum
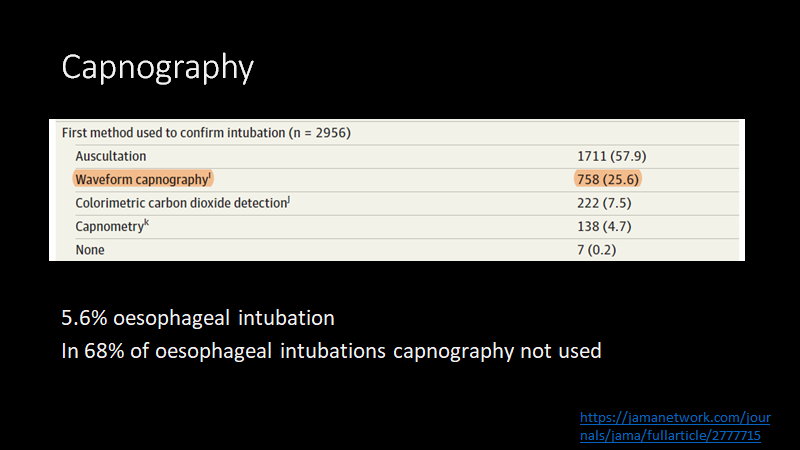
I'm confident capnography use is ingrained in UK clinical practice. A success of #NAP4 & the airway leads network
The low rates of capnography use in countries beyond the UK is a major cause of concern & a safety issue
@RussottoVin @ESICM @ASALifeline
As an addendum
I'm confident capnography use is ingrained in UK clinical practice. A success of #NAP4 & the airway leads network
The low rates of capnography use in countries beyond the UK is a major cause of concern & a safety issue
@RussottoVin @ESICM @ASALifeline

@MartinBromiley's tweet yesterday was very important here.
In his introduction to NAP4 Martin included this.
So let's be
-slow to judge others
-quick to learn ourselves
In his introduction to NAP4 Martin included this.
So let's be
-slow to judge others
-quick to learn ourselves
To trap undetected oesophageal intubation who is or is not up for this?
1/2
1/2
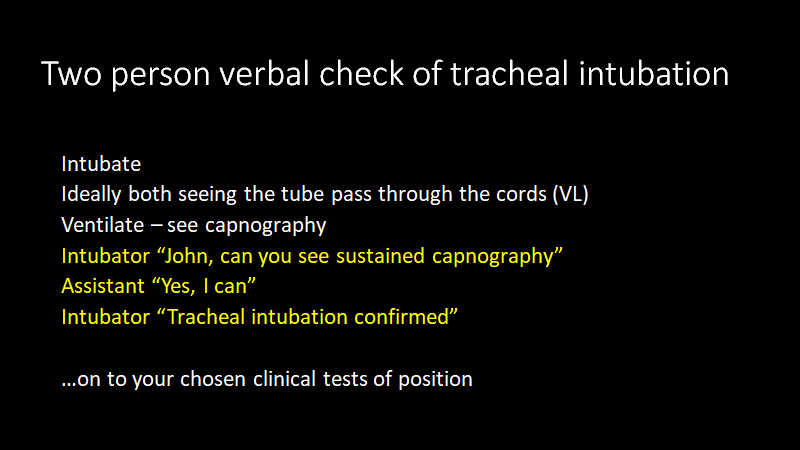
To trap undetected oesophageal intubation who is or is not up for a two person verbal check of capnography?
It would be great to see this re-tweeted so we can get a good number of votes to inform us of opinion.
Its a matter of professional importance
@dasairway @dastrainees @DAS_2021 @RCoANews @AAGBI @ICS_updates
Thanks
Its a matter of professional importance
@dasairway @dastrainees @DAS_2021 @RCoANews @AAGBI @ICS_updates
Thanks
جاري تحميل الاقتراحات...