


A few extra tips and tricks.
Don’t trust potassium.
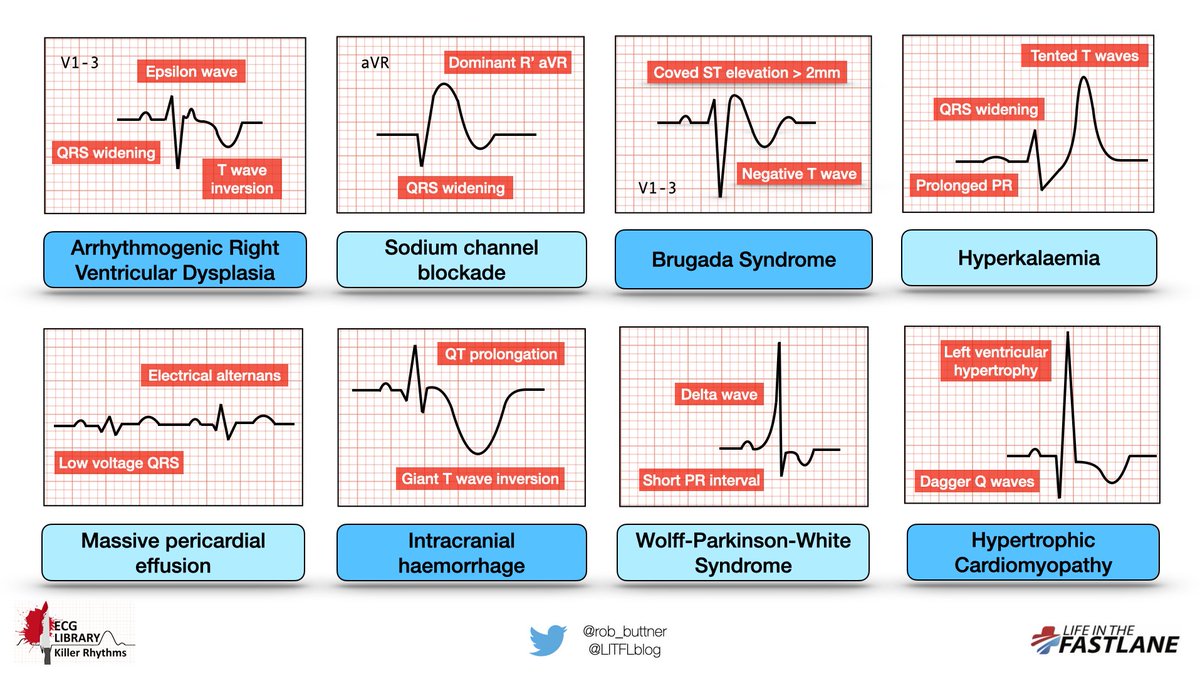
Patients can have a normal ECG right up until the point of hyperkalaemic PEA arrest. Any severely bradycardic patient has 👆🏾K until proven otherwise (1/6)
Don’t trust potassium.
Patients can have a normal ECG right up until the point of hyperkalaemic PEA arrest. Any severely bradycardic patient has 👆🏾K until proven otherwise (1/6)
Don’t get too tied up if you can’t find an Epsilon wave.
Although very specific, they are only present in about 50% of cases of ARVD. Look for other features such as right precordial QRS widening and TWI, and take clinical context into account (2/6)
Although very specific, they are only present in about 50% of cases of ARVD. Look for other features such as right precordial QRS widening and TWI, and take clinical context into account (2/6)

Patients with HCM can have a normal ECG. If clinical suspicion is high enough based on symptoms alone, refer for further work-up.
Beware of the apical variant which may present with giant TWI similar to that seen in ICH (3/6)
Beware of the apical variant which may present with giant TWI similar to that seen in ICH (3/6)
Cerebral T waves are mostly academic – hopefully you won’t be diagnosing massive ICH from the ECG.
Remember to always look at the patient in front of you - in this case, they will probably be unconscious! (4/6)
Remember to always look at the patient in front of you - in this case, they will probably be unconscious! (4/6)
Lastly, diagnosing a massive pericardial effusion from the ECG is pretty cool, but being able to identify one on bedside #echo is far cooler, and far more sensitive. This is a handy skill and should be part of every clinicians skillset (5/6)
ECG interpretation is essentially pattern recognition.
Take your skills to the next level by looking at as many ECGs as you can, following up on your patients after confirmatory testing (e.g. angiography), and checking out some of the excellent ECG blogs out there (6/6)
#FOAMed
Take your skills to the next level by looking at as many ECGs as you can, following up on your patients after confirmatory testing (e.g. angiography), and checking out some of the excellent ECG blogs out there (6/6)
#FOAMed

جاري تحميل الاقتراحات...