

#ثريد اليوم عن Bradycardia للمهتمين في المجال الصحي 💉
Bradycardia is a condition typically defined wherein an individual has a resting heart rate of under 60 beats per minute (BPM) in adults, although some studies use a heart rate of less than 50 BPM.
Bradycardia typically does not cause symptoms until the rate drops below 50 BPM
Bradycardia typically does not cause symptoms until the rate drops below 50 BPM
Types of bradycardia:
1- Sinus bradycardia is a type of slow heartbeat that originates from the sinus node of your heart. Your sinus node is often referred to as your heart’s pacemaker. It generates the organized electrical impulses that cause your heart to beat.
1- Sinus bradycardia is a type of slow heartbeat that originates from the sinus node of your heart. Your sinus node is often referred to as your heart’s pacemaker. It generates the organized electrical impulses that cause your heart to beat.
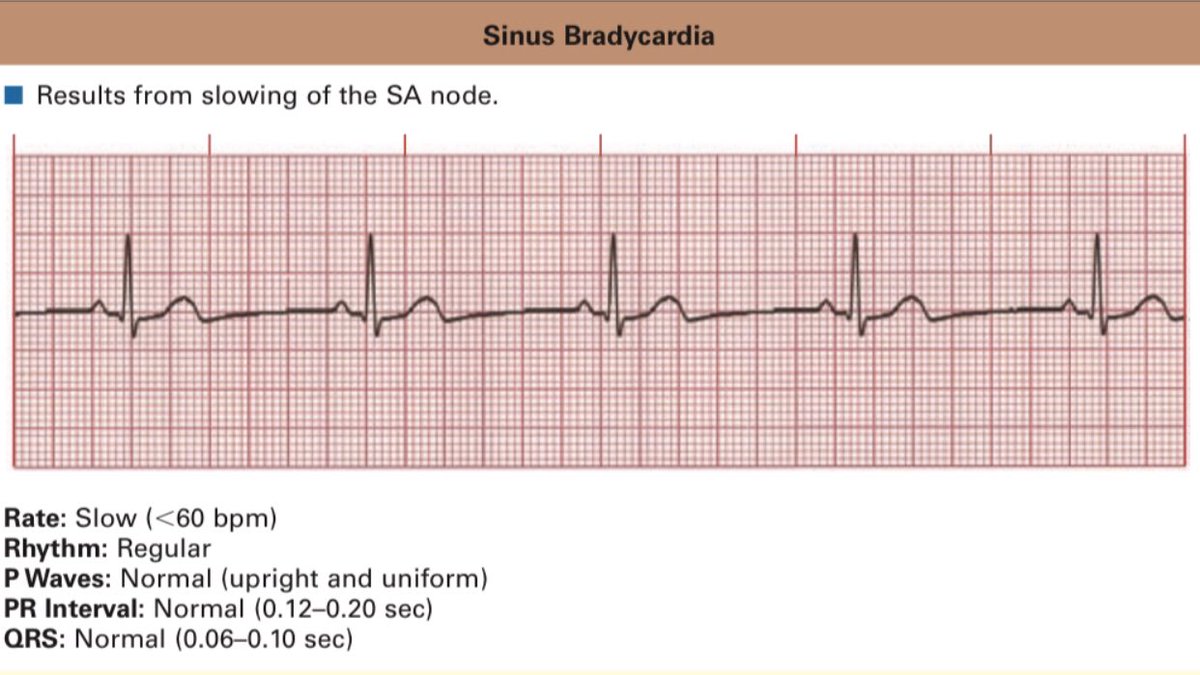
Note 📝 Sinus bradycardia is normal in athletes and during sleep.
In acute MI, it may be protective and beneficial or the slow rate may compromise cardiac output. Certain medications, such as beta blockers, may also cause sinus bradycardia.
In acute MI, it may be protective and beneficial or the slow rate may compromise cardiac output. Certain medications, such as beta blockers, may also cause sinus bradycardia.


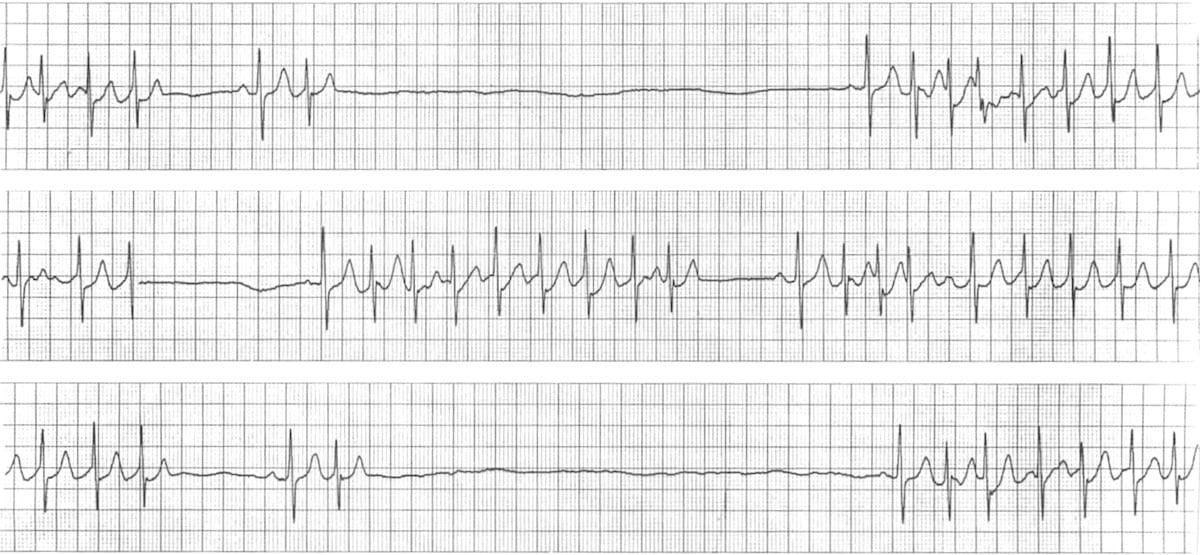
2- Sick sinus syndrome occurs when the sinus node (the heart's own pacemaker) fails and does not reliably trigger heartbeats. This is very common in elderly persons, but may occur at any age.

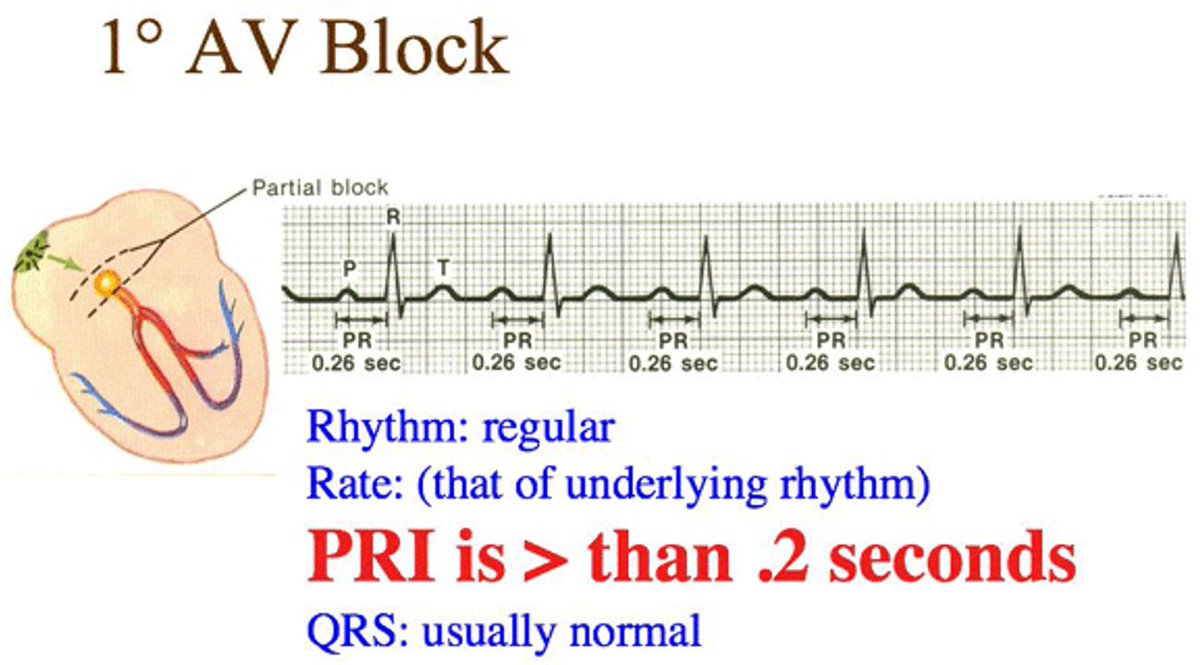
3- Heart block (AV) block is a complete or partial interruption of the electrical impulses on their way to the ventricles and results in a slow, unreliable heartbeat.Heart block may be present at birth, heart disease or due to age-related and tear on the heart's electrical system
Note 📝 Usually AV block is benign, but if associated with an acute MI, it may lead to further AV defects.
A- First-degree (AV) block is a condition of abnormally slow conduction through the AV node. It is defined by ECG changes that include a PR interval of greater than 0.20 without disruption of atrial to ventricular conduction. This condition is generally asymptomatic
Mobitz I type II AV block is a gradual prolongation of the PR interval over a few heart cycles until an atrial impulse is completely blocked, which manifest on the ECG as a P-wave not followed by a QRS complex. This cycle repeats itself over and over again.
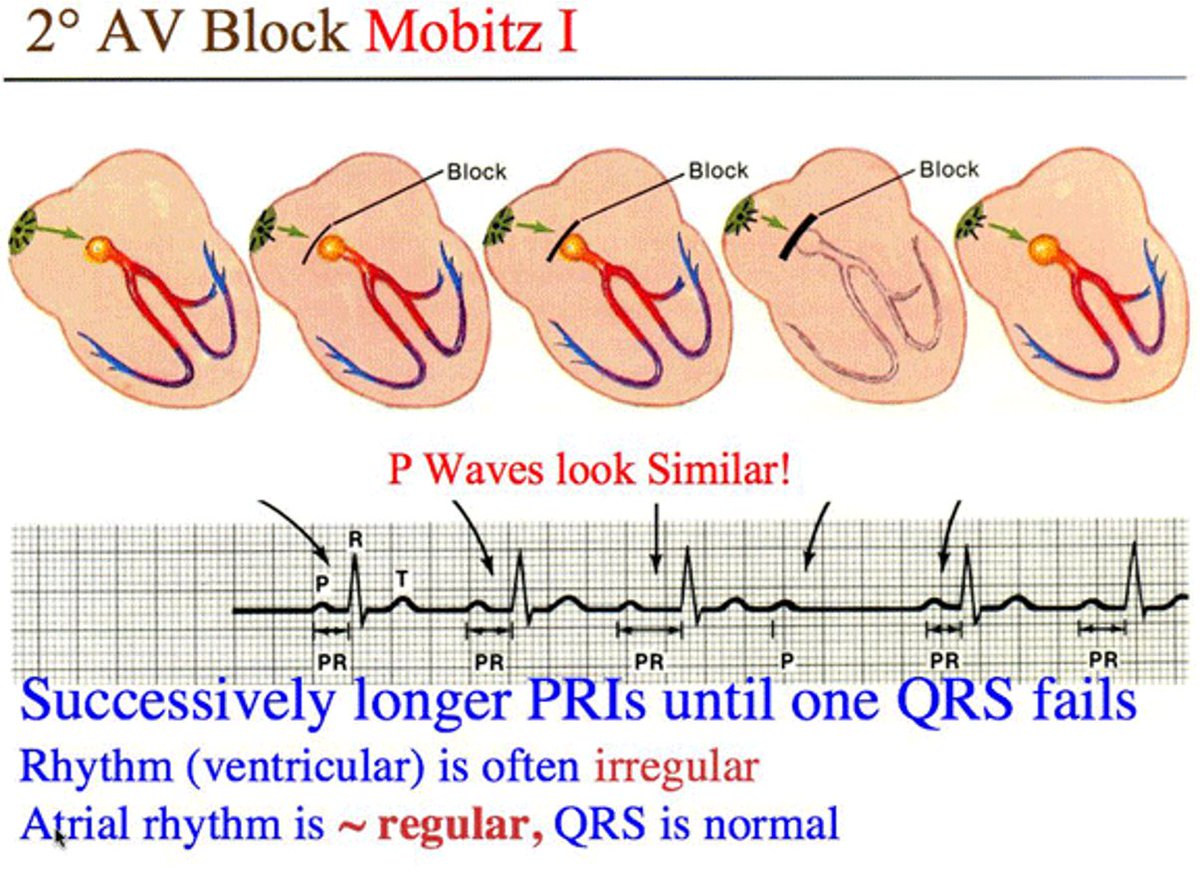
Note 📝 Mobitz I type II AV block may be caused by medication such as beta blockers, digoxin, and calcium channel blockers. Ischemia involving the right coronary artery is another cause.
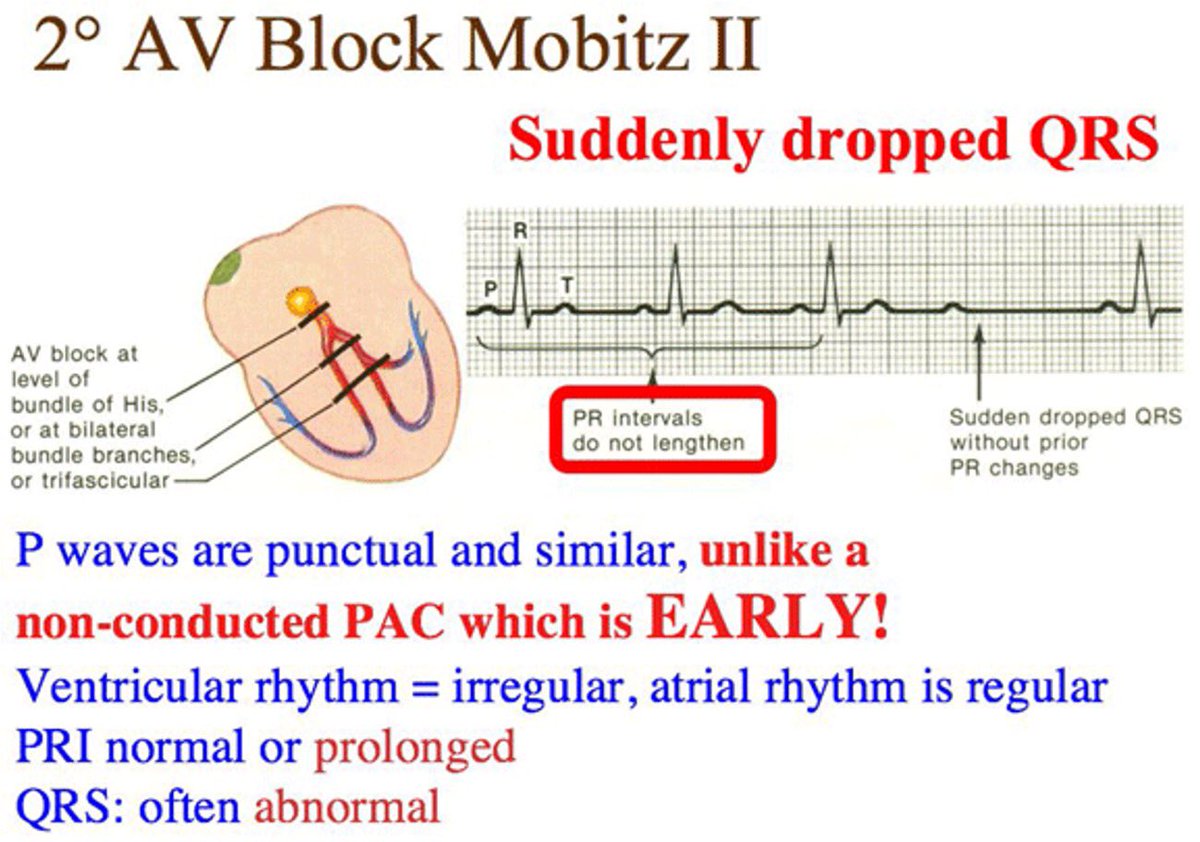
C- Mobitz II type II AV block is Consecutively conducted beats with the same PR interval are followed by a blocked sinus P wave. PR interval in the first beat after the block is similar to the PR interval before the AV block
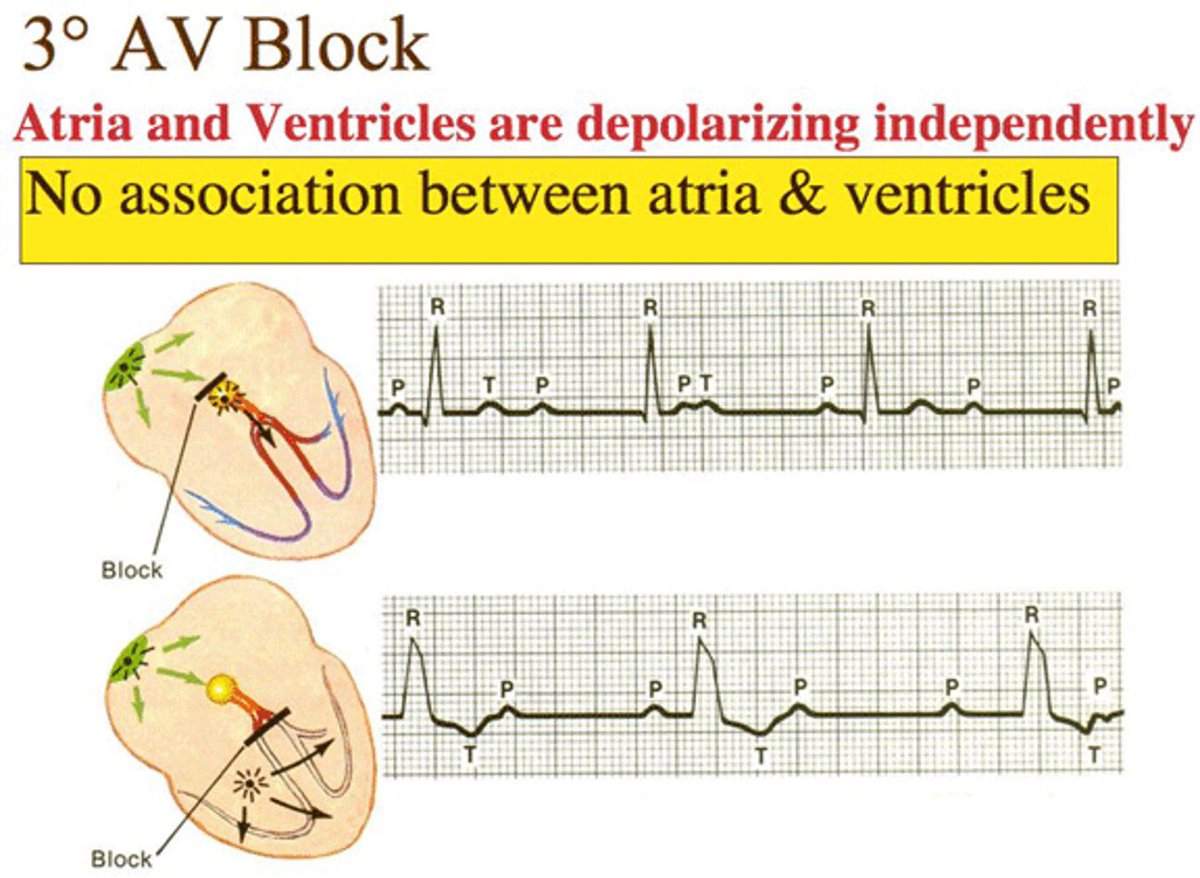
D-Third-degree AV block (complete heart block) exists when there are more P waves than QRS complexes, and there is no relationship between them (ie, no conduction). The conduction block may be at the level of the AVN, the bundle of His, or the bundle-branch Purkinje system.
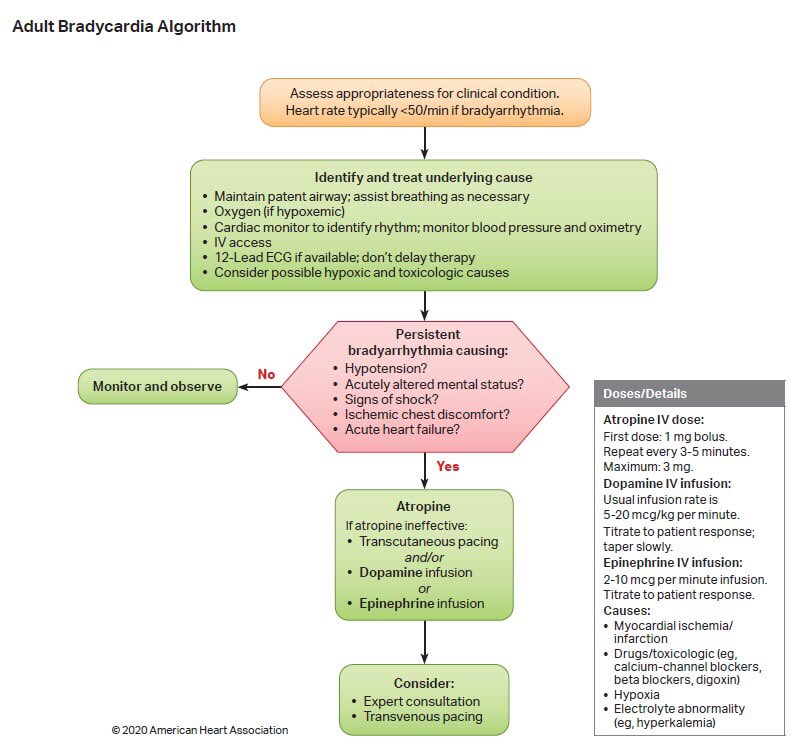
How to deal with bradycardia
1- Pulse rate 60 bpm?
2- persistent causes (hypotension, alter mental status, shock, chest pain, HF).
3- if yes Measure vital signs, including oxygen saturation.
4- Supply oxygen, begin cardiac monitoring, and start IV.
1- Pulse rate 60 bpm?
2- persistent causes (hypotension, alter mental status, shock, chest pain, HF).
3- if yes Measure vital signs, including oxygen saturation.
4- Supply oxygen, begin cardiac monitoring, and start IV.
5- administer atropine 0.5–1.0 mg IVP every 3–5 min, max. 0.03–0.04 mg/kg.
6- If patient remains symptomatic or has 2nd-degree (Mobitz type II) or 3rd-degree AV block, sedate patient and begin transcutaneous pacing, if available.
6- If patient remains symptomatic or has 2nd-degree (Mobitz type II) or 3rd-degree AV block, sedate patient and begin transcutaneous pacing, if available.
7- If no response, consider dopamine with continuous infusions (titrate to patient response) of 5–20 g/kg/min. Mix 400 mg/250 mL in normal saline, lactated Ringer’s solution, or D5W.
8- If patient is still hypotensive with severe bradycardia, consider epinephrine infusion, 2–10 g/min IV (add 1 mg of 1:1000 to 500 mL normal saline and infuse at 1–5 mL/min).
9- If still no response, consider isoproterenol, IV infusion: mix 1 mg in 250 mL normal saline, lactated Ringer’s solution, or D5W with rate of 2–10 g/min, titrate to patient response.
Note 📝 If patient is symptomatic, do not delay transcutaneous pacing while waiting for atropine to take effect or for IV access.
Use atropine with caution in a suspected acute MI; atropine may induce rate-related ischemia.
Use atropine with caution in a suspected acute MI; atropine may induce rate-related ischemia.
بكذا انتهى الثريد واتمنى انه عجبكم ❤️
جاري تحميل الاقتراحات...