

Tachycardia is the medical term for a heart rate over 100 beats per minute. There are many heart rhythm disorders (arrhythmias) that can cause tachycardia.
Sometimes, it's normal for you to have a fast heartbeat it’s called (sinus tachycardia) not over 120-130 bpm.
Sometimes, it's normal for you to have a fast heartbeat it’s called (sinus tachycardia) not over 120-130 bpm.

tachycardia can disrupt normal heart function and lead to serious complications, including:
1-Heart failure
2-Stroke
3-Sudden cardiac arrest or death
1-Heart failure
2-Stroke
3-Sudden cardiac arrest or death

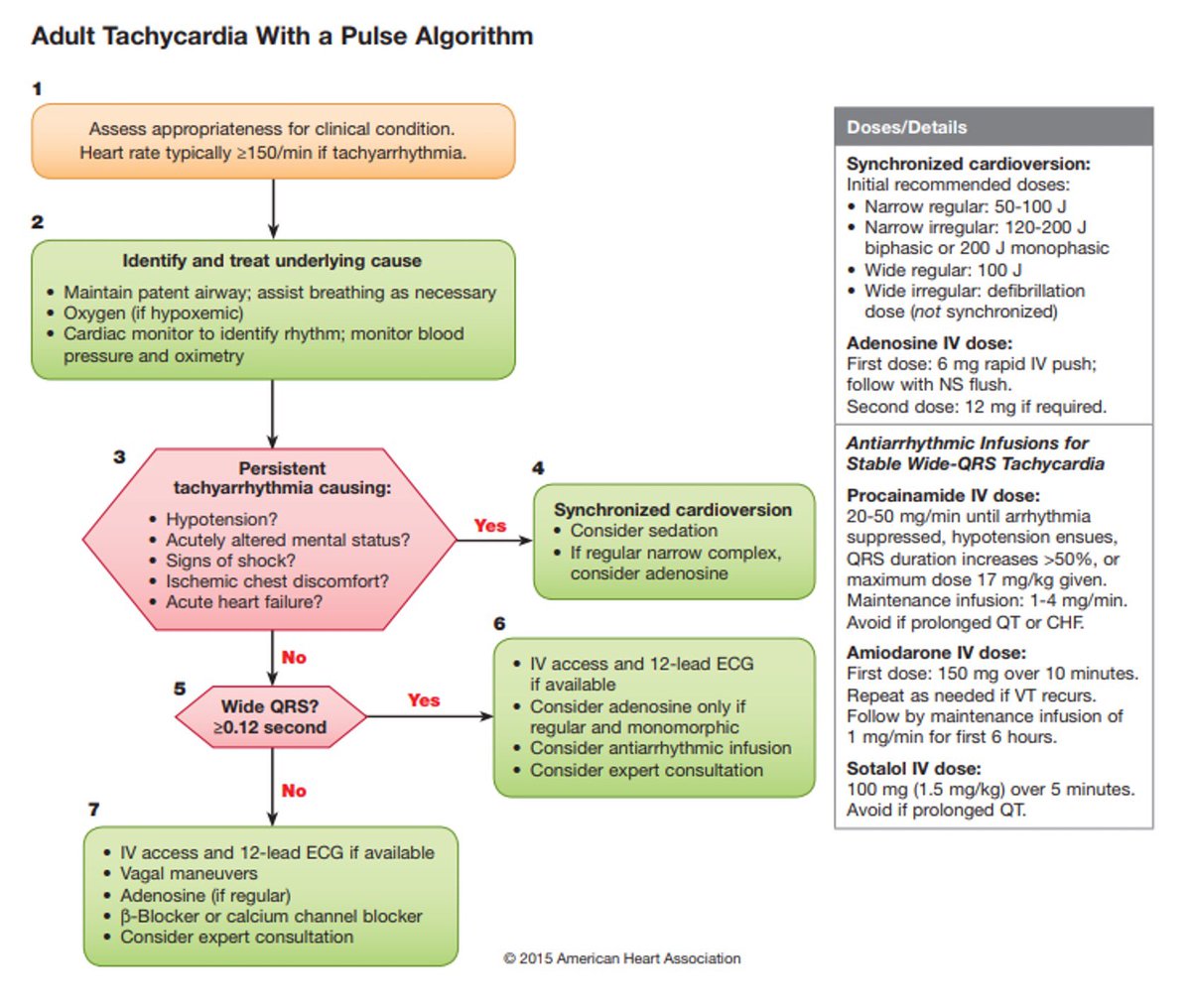
How to identify the tachycardia
1- look to rate
2- Assess the QRS Complex:
Narrow?:
Regular or Irregular
Wide QRS?:
Regular or Irregular
1- look to rate
2- Assess the QRS Complex:
Narrow?:
Regular or Irregular
Wide QRS?:
Regular or Irregular

Types of tachycardia
A-Narrow QRS tachycardia:
1. Sinus tachycardia
2. Supraventricular tachycardia (all the 3 below is types of SVT)+ proximal SVT.
3. Atrial flutter
4. Atrial fibrillation (irregular)
5. AV nodal reentry
A-Narrow QRS tachycardia:
1. Sinus tachycardia
2. Supraventricular tachycardia (all the 3 below is types of SVT)+ proximal SVT.
3. Atrial flutter
4. Atrial fibrillation (irregular)
5. AV nodal reentry
Wide QRS COMPLEX tachycardia:
1. Monomorphic VT (regular)
2. Polymorphic VT (irregular)
3. SVT with aberrancy
1. Monomorphic VT (regular)
2. Polymorphic VT (irregular)
3. SVT with aberrancy
1-Sinus tachycardia:
is an elevated sinus rhythm characterized by an increase in the rate of electrical impulses arising from the sinoatrial node, it’s also caused normally like in exercise, fever, Anemia, Hypotension, Blood loss and Exercise.
>>>>>>>
is an elevated sinus rhythm characterized by an increase in the rate of electrical impulses arising from the sinoatrial node, it’s also caused normally like in exercise, fever, Anemia, Hypotension, Blood loss and Exercise.
>>>>>>>
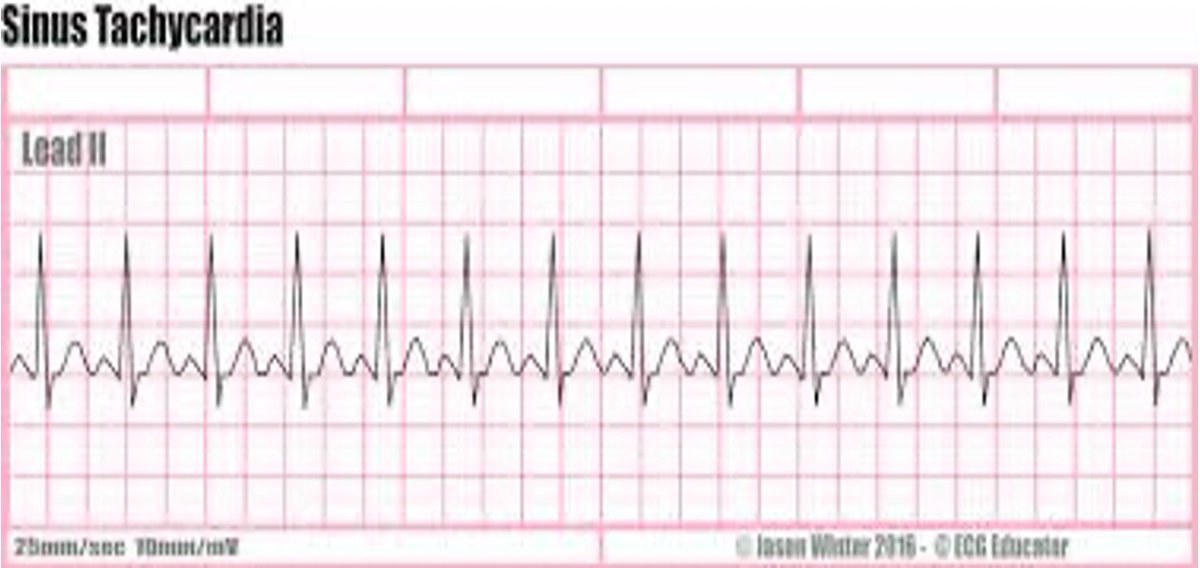
ECG findings in sinus tachycardia:
• P waves: Normal and upright
• QRS complex: Less than 0.12 second • Rate: more than 100 beats/minute
• Rhythm: Regular
• P-R interval: 0.12 to 0.20 second
Management: Treat causes
• P waves: Normal and upright
• QRS complex: Less than 0.12 second • Rate: more than 100 beats/minute
• Rhythm: Regular
• P-R interval: 0.12 to 0.20 second
Management: Treat causes
2- Proximal Supraventricular tachycardia (PSVT):
is an abnormally fast heart rhythm arising from improper electrical activity in the upper part of the heart (reentering of electrical pulse from the atria to ventricle).
>>>>>>>>
is an abnormally fast heart rhythm arising from improper electrical activity in the upper part of the heart (reentering of electrical pulse from the atria to ventricle).
>>>>>>>>
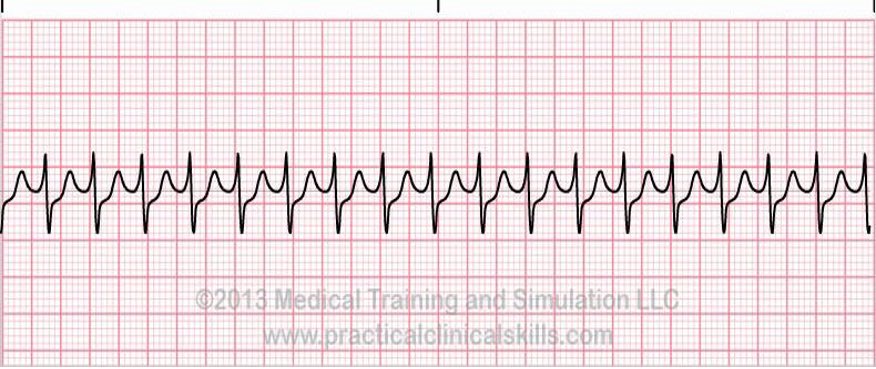
management:
If the patient is stable:
Vagal Maneuvers , Valsalva maneuver
Medication:
Adenosine: 6 mg rapid IV, if no conversion, give 12 mg IV (second dose) Diltiazem or verapamil (calcium channel blocker).
Stalol beta blocker 100mg or 1.5/kg over 5 min avoid it if prolonged QT
If the patient is stable:
Vagal Maneuvers , Valsalva maneuver
Medication:
Adenosine: 6 mg rapid IV, if no conversion, give 12 mg IV (second dose) Diltiazem or verapamil (calcium channel blocker).
Stalol beta blocker 100mg or 1.5/kg over 5 min avoid it if prolonged QT
If unstoppable:
Cardioversion 50-100J, consider adenosine and consultation.
Cardioversion 50-100J, consider adenosine and consultation.
3- Atrial flutter :
The result of a rapid atrial reentry focus
Manifests as:
2 : 1 atrioventricular conduction ratio (50% of the atrial impulses are conducted through the ventricles) 3 : 1 4 : 1
The result of a rapid atrial reentry focus
Manifests as:
2 : 1 atrioventricular conduction ratio (50% of the atrial impulses are conducted through the ventricles) 3 : 1 4 : 1

Management:
If stable pt:
-Beta blockers (stalol 100mg or 1.5/kg over 5 min avoid it if prolonged QT). -Calcium channel blocking agents used in caution with:
Congestive heart failure, Asthma, COPD
-Digoxin
Synchronized shock of 50 J (initial attempt) to 100 J.
If stable pt:
-Beta blockers (stalol 100mg or 1.5/kg over 5 min avoid it if prolonged QT). -Calcium channel blocking agents used in caution with:
Congestive heart failure, Asthma, COPD
-Digoxin
Synchronized shock of 50 J (initial attempt) to 100 J.
4- Atrial fibrillation:
is a quivering or irregular heartbeat (arrhythmia) that can lead to blood clots, stroke, heart failure and other heart-related complications.
is a quivering or irregular heartbeat (arrhythmia) that can lead to blood clots, stroke, heart failure and other heart-related complications.

Management:
If stable pt:
Beta blockers (stalol 10mg or 1,5/kg over 5 min avoid it if prolonged QT) -Calcium channel blocking agents used in caution with:
Congestive heart failure, Asthma, COPD
-Digoxin
If unstable pt:
Synchronized shock of 100 to 120 J biphasic (200 J monophasic
If stable pt:
Beta blockers (stalol 10mg or 1,5/kg over 5 min avoid it if prolonged QT) -Calcium channel blocking agents used in caution with:
Congestive heart failure, Asthma, COPD
-Digoxin
If unstable pt:
Synchronized shock of 100 to 120 J biphasic (200 J monophasic
5- Monomorphic VT:
Very broad QRS complexes (>200 ms) with uniform morphology.
Very broad QRS complexes (>200 ms) with uniform morphology.
Management:
If stable pt:
Amiodarone 150 mg IV over 10 minutes
Procainamide 20-50 mg (alternative drug) avoid it if prolong QT, CHF
If unstable pt:
synchronized cardioversion Begin with 100 J, If no response, dose should be increased at 200 J, 300 J, and 360 J monophasic
If stable pt:
Amiodarone 150 mg IV over 10 minutes
Procainamide 20-50 mg (alternative drug) avoid it if prolong QT, CHF
If unstable pt:
synchronized cardioversion Begin with 100 J, If no response, dose should be increased at 200 J, 300 J, and 360 J monophasic
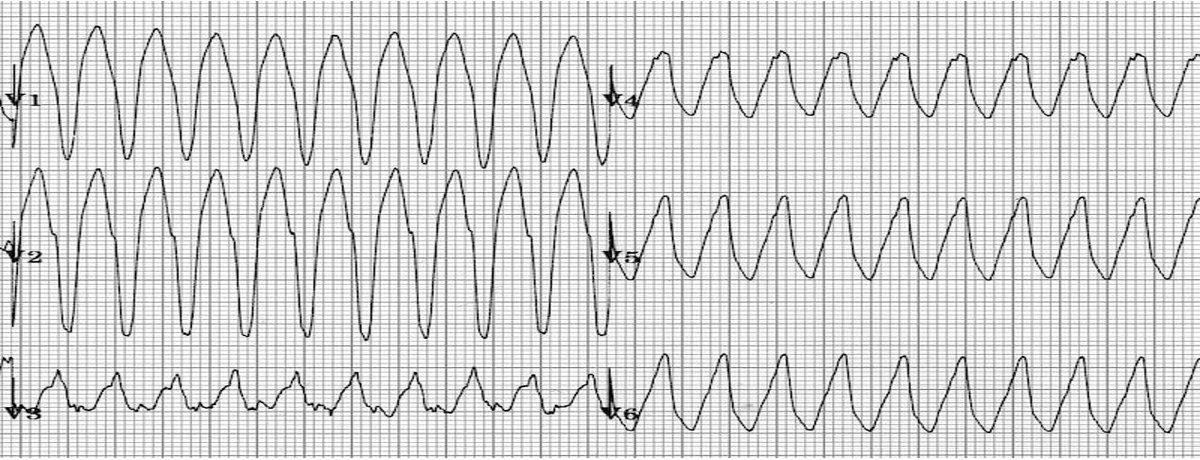
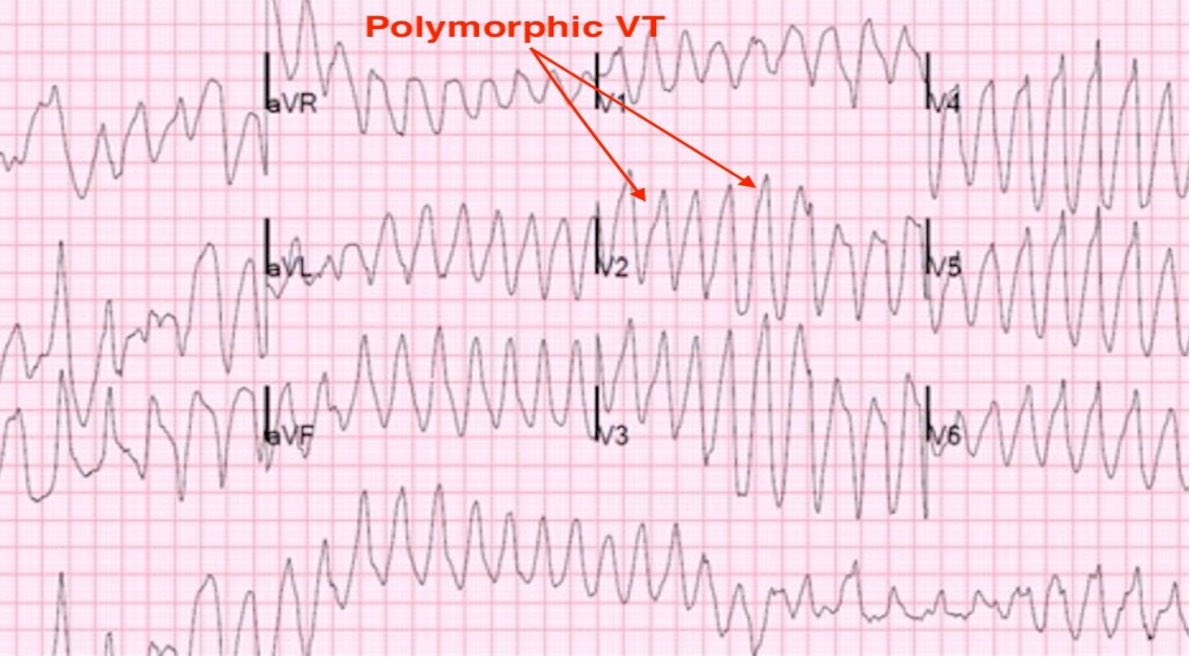
6- Polymorphic VT:
is a form of ventricular tachycardia in which there are multiple ventricular foci with the resultant QRS complexes varying in amplitude, axis and duration. The commonest cause of PVT is myocardial ischemia.
Polymorphic VT can degenerate into VF
is a form of ventricular tachycardia in which there are multiple ventricular foci with the resultant QRS complexes varying in amplitude, axis and duration. The commonest cause of PVT is myocardial ischemia.
Polymorphic VT can degenerate into VF
Management:
Treated as ventricular fibrillation High-energy unsynchronized shocks
Treated as ventricular fibrillation High-energy unsynchronized shocks
Torsades de points:
is a specific form of polymorphic ventricular tachycardia occurring in the context of QT prolongation; it has a characteristic morphology in which the QRS complexes “twist” around the isoelectric line.
Rhythm may be result of prolonged Q-T interval.
is a specific form of polymorphic ventricular tachycardia occurring in the context of QT prolongation; it has a characteristic morphology in which the QRS complexes “twist” around the isoelectric line.
Rhythm may be result of prolonged Q-T interval.

Management:
Medications that prolong Q-T interval should be discontinued. Electrolyte imbalances should be corrected
IV magnesium sulfate should be given
Medications that prolong Q-T interval should be discontinued. Electrolyte imbalances should be corrected
IV magnesium sulfate should be given
بكذا انتهى الثريد وانشاء الله نال على اعجابكم 🙏❤️
جاري تحميل الاقتراحات...