

الى الزملاء في مجال التغذية العلاجية
يومكم سعيد ✨
مع تزايد حالات الاصابة وزيادة ضغط الحالات الحرجة ، شعرت ان اليوم هو الوقت المناسب لمشاركتكم بعض المعلومات والتي تخص التدخل الغذائي العلاجي لمرضى #COVID19
وخاصة في critical stages
هل لنا تدخل حاسم ! خلينا نشوف 👌🏼✨
يومكم سعيد ✨
مع تزايد حالات الاصابة وزيادة ضغط الحالات الحرجة ، شعرت ان اليوم هو الوقت المناسب لمشاركتكم بعض المعلومات والتي تخص التدخل الغذائي العلاجي لمرضى #COVID19
وخاصة في critical stages
هل لنا تدخل حاسم ! خلينا نشوف 👌🏼✨
في البداية
اذا كان المريض قادرة على تناول الغذاء orally
Energy and protein enriched diet
ملاحظة📝
لان الاعراض التنفسية تجعل تناول الطعام مجهد الافضل يكون Soft/full liquid diet
(oral nutritional supplement (ONS)(400
- kcal/day including 30 g or more of protein/day)
اذا كان المريض قادرة على تناول الغذاء orally
Energy and protein enriched diet
ملاحظة📝
لان الاعراض التنفسية تجعل تناول الطعام مجهد الافضل يكون Soft/full liquid diet
(oral nutritional supplement (ONS)(400
- kcal/day including 30 g or more of protein/day)
- احب انوه ان تقريبا من ٨٠-٩٠٪ من مرضى #COVID19 ذو الحالات الحرجة
على Entral nutrition حيث ان حالتهم الصحية تمنعهم من تناول ٥٠٪ من احتياجهم وبذلك يكون entral nutrition هو أفضل خيار متاح
ملاحظة 📝
- ( We will start within 24-48 hours)
على Entral nutrition حيث ان حالتهم الصحية تمنعهم من تناول ٥٠٪ من احتياجهم وبذلك يكون entral nutrition هو أفضل خيار متاح
ملاحظة 📝
- ( We will start within 24-48 hours)
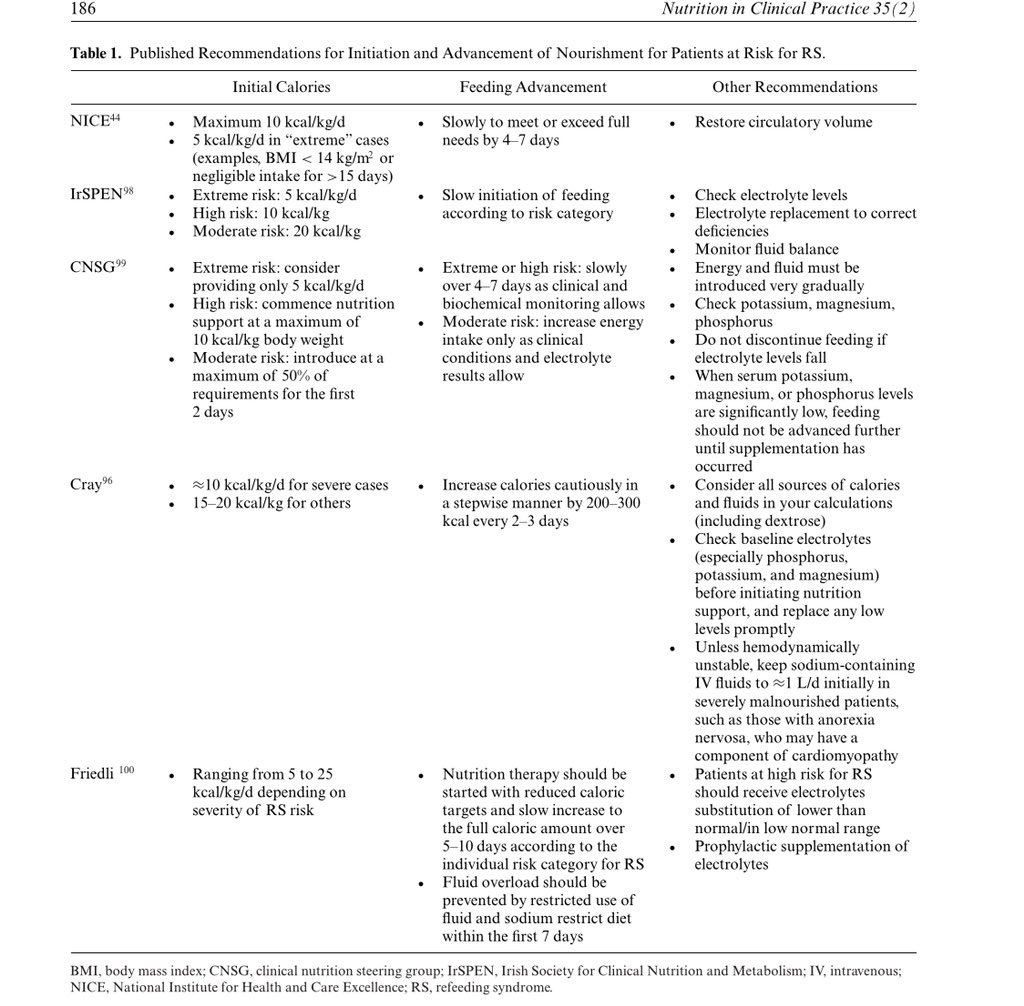
ناخذ فالاعتبار refeeding syndrome نلاحظ PO4, Mg and K+ ونكون واعين في هذه الحالة
ونتبع البرتوكول الخاص بذلك
ونتبع البرتوكول الخاص بذلك
عند البدا بال
entral nutrition
القاعدة (start low advance slowly )-
ملاحظة 📝 مهمة
•If the patient , ECMO ,vasopressin
meditation
hypocaloric or trophic feeding -10-20 ml/h)
•When the patient stable- advancing to full dose EN slowly over the first week.
entral nutrition
القاعدة (start low advance slowly )-
ملاحظة 📝 مهمة
•If the patient , ECMO ,vasopressin
meditation
hypocaloric or trophic feeding -10-20 ml/h)
•When the patient stable- advancing to full dose EN slowly over the first week.
نحسب الاحتياجات على مراحل👌🏼
Energy needs:
- 15-20 kcal/kg /day (which should be 70-80% of caloric requirements)
- Recommend after day 5 provide 25 kcal/kg /day (and up to 30 kcal/kg/day for severely unwell patients).
Energy needs:
- 15-20 kcal/kg /day (which should be 70-80% of caloric requirements)
- Recommend after day 5 provide 25 kcal/kg /day (and up to 30 kcal/kg/day for severely unwell patients).
ABW used for patients of normal weight, and an adjusted BW for overweight and obese patients.
• Protein needs:
- 1.2-2.0 gm/kg ABW/day1 - “For obese patient: 1.3 g/kg adjusted BW”
• Protein needs:
- 1.2-2.0 gm/kg ABW/day1 - “For obese patient: 1.3 g/kg adjusted BW”
دائما ما تسمع كلمة متكررة اثناء الراوند (negative balance our target)✨
نحتاج نوازن بين restrictive fluid و
and meeting nutrition targets
• لذلك Consider 1.3-1.5 kcal/ml formula خيار مثالي 👌🏼
📝 اذا كان المريض على propofol
, (1.1*ml*24) لا تنسى تحسب الكلوري
نحتاج نوازن بين restrictive fluid و
and meeting nutrition targets
• لذلك Consider 1.3-1.5 kcal/ml formula خيار مثالي 👌🏼
📝 اذا كان المريض على propofol
, (1.1*ml*24) لا تنسى تحسب الكلوري
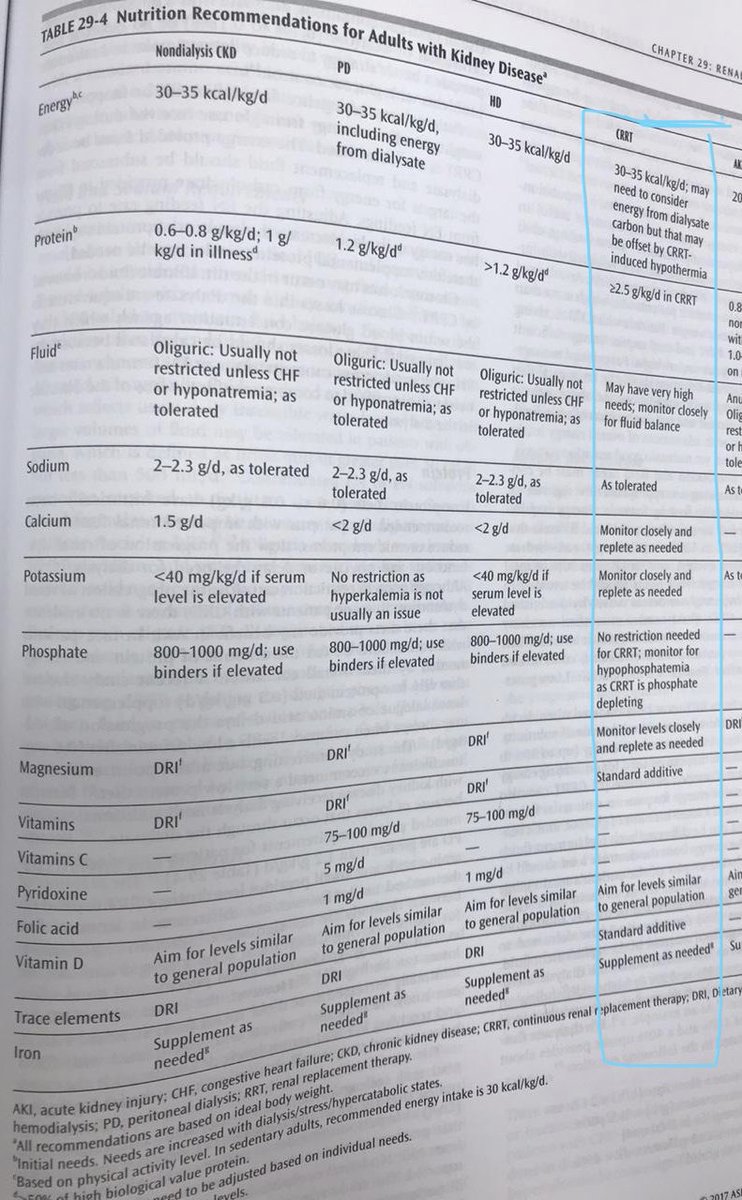
بالنسبة لل laboratories راح نلاحظ ان فيه تدهور ملحوظ عند كثير من المرضى فيما يخص renal profile
- في حال كان المريض على CRRT وكان Stable نتبع كمية البروتين الخاصة بذلك
- ولكن في حال كان المريض في حالة unstable - وهذا في اغلب الاحيان - نتبع التدرج المذكور فالاعلى
- في حال كان المريض على CRRT وكان Stable نتبع كمية البروتين الخاصة بذلك
- ولكن في حال كان المريض في حالة unstable - وهذا في اغلب الاحيان - نتبع التدرج المذكور فالاعلى
- عند ارتفاع Na نقوم برفع water flushing ويتم مناقشة ذلك من الفريق لهدف عدم الاخلال negative balance
- احيانا يكون normal saline مستعمل في تجهيز بعض الادوية قد نقترح استعمال D5 بدل ذلك واذا كان DM PT يكون على
- sliding scale or IV Insulin infusion
📝اختر formula قليلة Na
- احيانا يكون normal saline مستعمل في تجهيز بعض الادوية قد نقترح استعمال D5 بدل ذلك واذا كان DM PT يكون على
- sliding scale or IV Insulin infusion
📝اختر formula قليلة Na
A standard high protein (> 20% protein) polymeric isotonic enteral formula should be used in the early acute phase of critical illness.
• Avoid ❌dense formula (2.0 kcal/ml)- increase enteral feeding intolerance (EFI).
• Avoid ❌dense formula (2.0 kcal/ml)- increase enteral feeding intolerance (EFI).
Gastric residual volume (GRV)
لا تطلب عمل GRV بكثرة لانه ممكن يزيد تعريض الفريق للعدوى ، وفي حال تم ذلك بدون طلبك
•, use threshold off 300-500 ml with less frequent
وقف القياس اذا
GRVs have been less than 300ml for > 48 hours
لا تطلب عمل GRV بكثرة لانه ممكن يزيد تعريض الفريق للعدوى ، وفي حال تم ذلك بدون طلبك
•, use threshold off 300-500 ml with less frequent
وقف القياس اذا
GRVs have been less than 300ml for > 48 hours
يمكن تقييم
عن طريق intolerance
( daily physical examination and
confirmation of stool passage and gas. abdominal destination state)
For(EFI):بالبداية
• Use fiber free formula- reattempt fiber after GI improves.
• Use of a prokinetic agent Metoclopramide ، erythromycin.etc
عن طريق intolerance
( daily physical examination and
confirmation of stool passage and gas. abdominal destination state)
For(EFI):بالبداية
• Use fiber free formula- reattempt fiber after GI improves.
• Use of a prokinetic agent Metoclopramide ، erythromycin.etc
• وفي حال الاستمرار EFI
o Post pyloric EN
متى تجي اللحظة الي نوقف فيها EN تماما !؟
• Hemodynamic instability requiring vasopressor support at high or escalating doses.
• Patients on multiple vasopressor agents.
• Rising lactate levels.
•Gastrointestinal dysfunctions
o Post pyloric EN
متى تجي اللحظة الي نوقف فيها EN تماما !؟
• Hemodynamic instability requiring vasopressor support at high or escalating doses.
• Patients on multiple vasopressor agents.
• Rising lactate levels.
•Gastrointestinal dysfunctions
EN may be initiated/restarted after the patient is adequately resuscitated and/or has been on a stable vasopressor dose with sustained mean arterial pressure of >65 mmHg
ممكن نحتاج نتجه ناحية PN في حال كان المريض stable لكن المسالة GI dysfunctions
نتناقش مع الفريق واتخذ الخطوة👌🏼
ممكن نحتاج نتجه ناحية PN في حال كان المريض stable لكن المسالة GI dysfunctions
نتناقش مع الفريق واتخذ الخطوة👌🏼
المعلومات الي موجودة في كامل التغريدات استفدت من زملاء ومن خبرة بسيطة و ايضا من مراجع وتجميعها بعض الزملاء .
اي معلومات اضافية راح تسعدني 🤍✨
اي معلومات اضافية راح تسعدني 🤍✨
جاري تحميل الاقتراحات...