

Glad you enjoyed my 1st #neuro #tweetorial on dizziness!
Let’s cover another neuroanatomy-based approach to clinical diagnosis topic: nerves and muscles of the arm and hand.
#Neurology #MedEd #MedStudentTwitter @CPSolvers @Tracey1milligan @MadSattinJ @MedTweetorials @DxRxEdu
1
Let’s cover another neuroanatomy-based approach to clinical diagnosis topic: nerves and muscles of the arm and hand.
#Neurology #MedEd #MedStudentTwitter @CPSolvers @Tracey1milligan @MadSattinJ @MedTweetorials @DxRxEdu
1
In med school, we often start off by learning the brachial plexus–complicated! It's not that common to need to conjure it up for clinical dx.
So let’s start with just 5 major nerves to the arm and hand, and come back to the plexus in a separate tweetorial for neuro geeks!
2/
So let’s start with just 5 major nerves to the arm and hand, and come back to the plexus in a separate tweetorial for neuro geeks!
2/
Those 5 nerves are:
Musculocutaneous
Axillary
Radial
Median
Ulnar
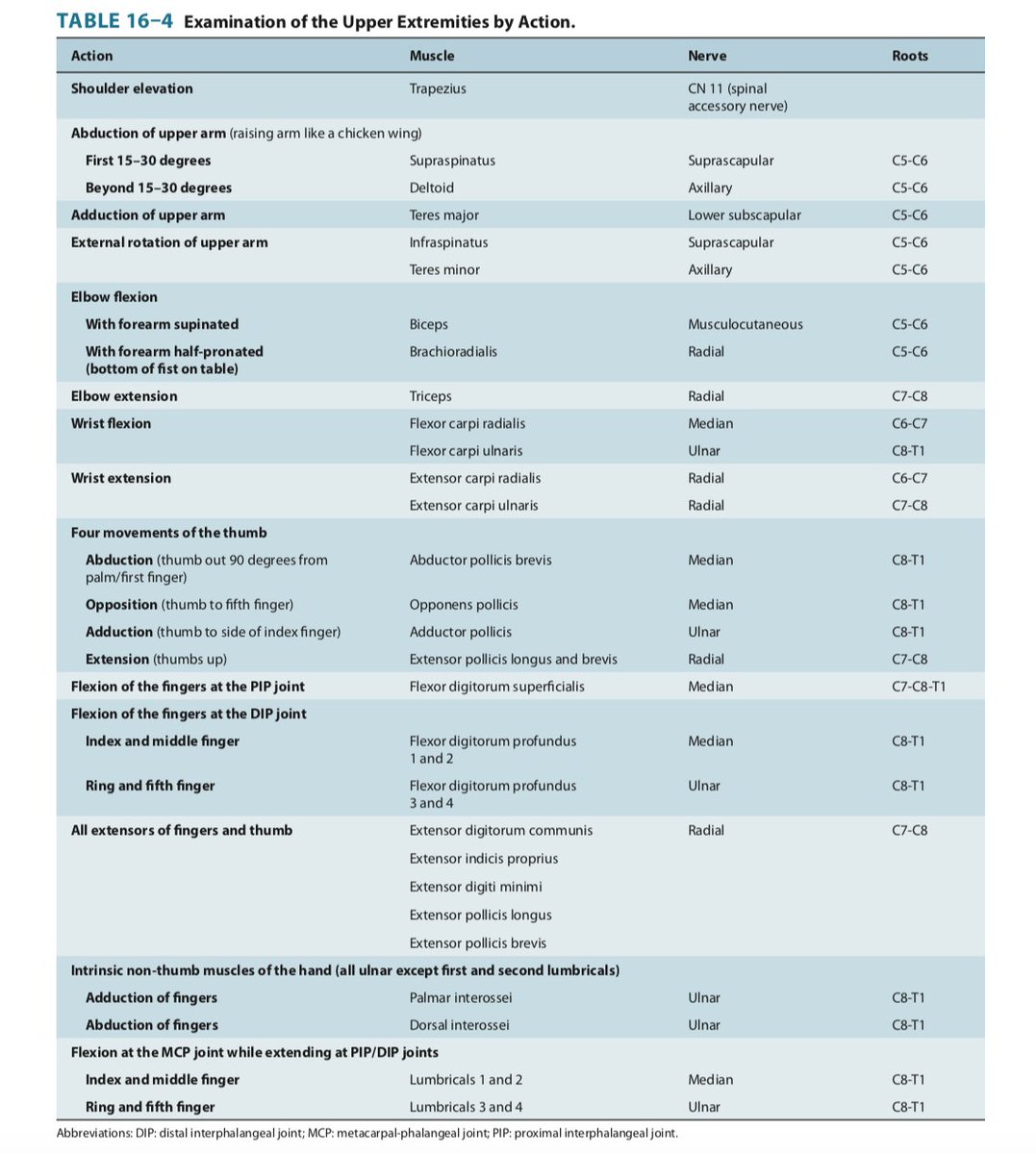
What’s most important to know about each nerve is:
- the muscles it supplies and their actions
- the sensory territories it supplies
3/
Musculocutaneous
Axillary
Radial
Median
Ulnar
What’s most important to know about each nerve is:
- the muscles it supplies and their actions
- the sensory territories it supplies
3/
If you know these 2 elements for each of the above 5 nerves, you can diagnose most peripheral issues of the arm/hand!
If you can't figure it out with just this information, you may be dealing with a radiculopathy or plexopathy!
4/
If you can't figure it out with just this information, you may be dealing with a radiculopathy or plexopathy!
4/
Let’s knock out the easy ones first musculocutaneous and axillary: they innervate just a few muscles, ALL above the elbow!
MUSCULOCUTANEOUS innervates 2 muscles:
- Biceps: elbow flexion
(Brachialis: not really clinically relevant)
Sensory: lateral forearm
5/
MUSCULOCUTANEOUS innervates 2 muscles:
- Biceps: elbow flexion
(Brachialis: not really clinically relevant)
Sensory: lateral forearm
5/
AXILLARY innervates 2 muscles
- Deltoid: abduction of upper arm >30 degrees ("chicken wing." (Supraspinatus does first ~ 30 degrees)
- Teres minor: external rotation of upper arm
Sensory: outer upper arm
6/
- Deltoid: abduction of upper arm >30 degrees ("chicken wing." (Supraspinatus does first ~ 30 degrees)
- Teres minor: external rotation of upper arm
Sensory: outer upper arm
6/
It’s rare to have an isolated musculocutaneous or axillary neuropathy (can occur with shoulder trauma or from surgical positioning).
So if the muscles supplied by these nerves are affected, look for other affected muscles that could implicate a radiculopathy or plexopathy!
7/
So if the muscles supplied by these nerves are affected, look for other affected muscles that could implicate a radiculopathy or plexopathy!
7/
Those 2 were pretty easy, but also less clinically relevant.
Now we move into the more complicated nerves that are also much more commonly affected clinically.
But let's keep the big picture principles for diagnosis/localization in mind as we go!
8/
Now we move into the more complicated nerves that are also much more commonly affected clinically.
But let's keep the big picture principles for diagnosis/localization in mind as we go!
8/
RADIAL: lots muscles of arm, forearm and hand (but no intrinsic hand muscles), but there's a Mnemonic:
Radial nerve is the BEST
Brachioradialis (flexion of elbow when half-pronated
Extensors of forearm, wrist, fingers, thumb
Supinator
Triceps (another Extensor: of elbow)
9/
Radial nerve is the BEST
Brachioradialis (flexion of elbow when half-pronated
Extensors of forearm, wrist, fingers, thumb
Supinator
Triceps (another Extensor: of elbow)
9/
RADIAL big picture = posterior compartment of the arm: elbow, wrist, finger, and thumb extension
...with 2 exceptions:
Brachioradialis: similar action to biceps except with forearm turned so thumb is up
Supinator: supination of forearm (turning forearm/hand to present SoUP
10
...with 2 exceptions:
Brachioradialis: similar action to biceps except with forearm turned so thumb is up
Supinator: supination of forearm (turning forearm/hand to present SoUP
10
Radial Sensory:
Posterior/lateral upper arm
Posterior forearm
Dorsum of thumb, index, middle and lateral half of ring (except nail beds of index, middle, and lateral half of ring = median); medial half of ring + pinky = ulnar
So just like motor: sensory= posterior/dorsum
11/
Posterior/lateral upper arm
Posterior forearm
Dorsum of thumb, index, middle and lateral half of ring (except nail beds of index, middle, and lateral half of ring = median); medial half of ring + pinky = ulnar
So just like motor: sensory= posterior/dorsum
11/
Radial neuropathy -> WRIST DROP: weakness of wrist and finger extension.
Radial nerve compression at axilla (e.g., 2/2 crutches) also causes triceps weakness
Radial nerve compression at spiral groove (humerus fracture, or "Sat PM palsy") affects B-E-S, spares Triceps
12/
Radial nerve compression at axilla (e.g., 2/2 crutches) also causes triceps weakness
Radial nerve compression at spiral groove (humerus fracture, or "Sat PM palsy") affects B-E-S, spares Triceps
12/
Pearl: **Pseudo-Radial**
Upper motor neuron hand/arm weakness 2/2 CNS lesion (in hand knob of motor cortex) preferentially affects extensors (incl triceps) and supinator (hence pronator drift):
PSEUDOradial palsy= central fake-out for peripheral!
13/
Upper motor neuron hand/arm weakness 2/2 CNS lesion (in hand knob of motor cortex) preferentially affects extensors (incl triceps) and supinator (hence pronator drift):
PSEUDOradial palsy= central fake-out for peripheral!
13/
Pearl:
If you relax your hand into wrist drop position, you'll see it's harder to abduct/adduct the fingers than with wrist neutral.
Don't be fooled into thinking that interossei (ulnar!) weakness accompanies wrist drop: lay hand flat and test abduction/adduction that way!
14
If you relax your hand into wrist drop position, you'll see it's harder to abduct/adduct the fingers than with wrist neutral.
Don't be fooled into thinking that interossei (ulnar!) weakness accompanies wrist drop: lay hand flat and test abduction/adduction that way!
14
So in sum, for radial, it does stuff in the posterior arm/forearm/hand + brachioradialis/supinator!
It's the BEST!
Brachioradialis (flexion of elbow when half-pronated
Extensors of forearm, wrist, fingers, thumb
Supinator
Triceps (another Extensor: of elbow)
15/
It's the BEST!
Brachioradialis (flexion of elbow when half-pronated
Extensors of forearm, wrist, fingers, thumb
Supinator
Triceps (another Extensor: of elbow)
15/
MEDIAN and ULNAR
- Nothing above the elbow
- A few things in the forearm
- LOTS in the hand
In general:
- Median does thumb-side; Ulnar does pinky side, but there are exceptions
16/
- Nothing above the elbow
- A few things in the forearm
- LOTS in the hand
In general:
- Median does thumb-side; Ulnar does pinky side, but there are exceptions
16/
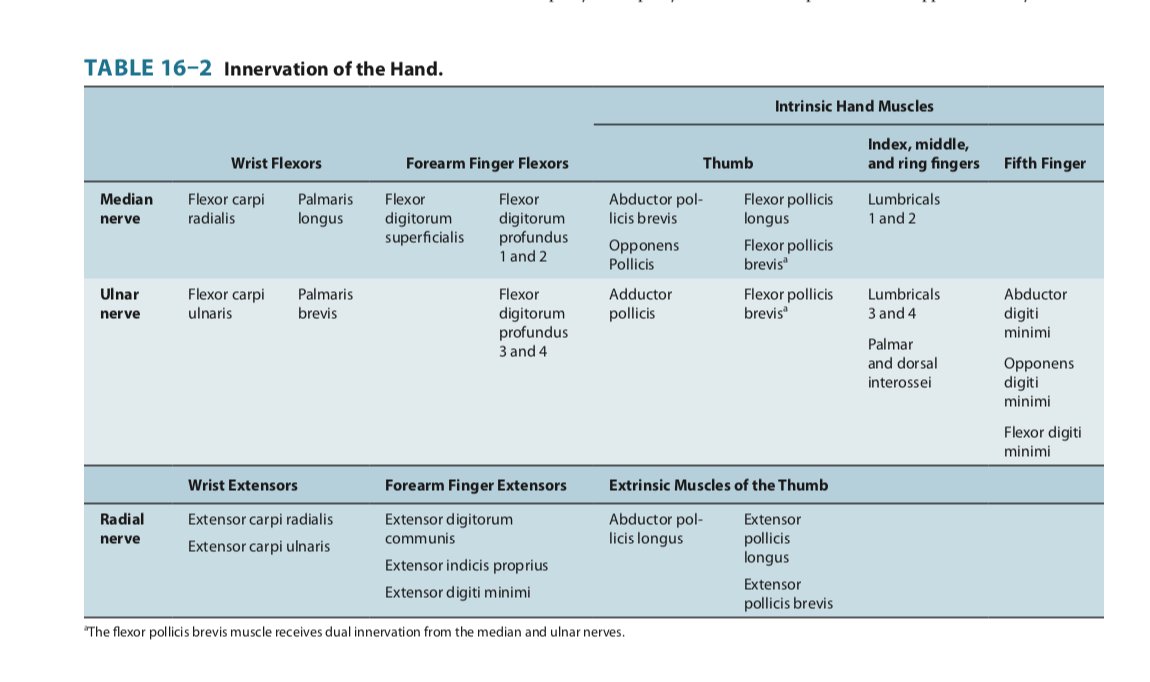
What obeys this split rule?
- Wrist flexors: Flexor carpi: radialis (median) vs Ulnaris (ulnar)
- Lumbricals (flex extended fingers at MCP): 1&2 (median) vs 3&4(ulnar)
- Flexor digitorum profundus (flexes at DIP): 1&2 (median) vs 3&4(ulnar)
- Sensory (see fig)
17/
- Wrist flexors: Flexor carpi: radialis (median) vs Ulnaris (ulnar)
- Lumbricals (flex extended fingers at MCP): 1&2 (median) vs 3&4(ulnar)
- Flexor digitorum profundus (flexes at DIP): 1&2 (median) vs 3&4(ulnar)
- Sensory (see fig)
17/

What does NOT obey this split rule:
- Flexor digitorum superficialis (flexion at PIP): ALL median
- Interossei (dorsal abduct fingers; palmar adduct fingers): ALL ulnar
- Median does pronators
- Thumb: lots happening see next tweet!
18/
- Flexor digitorum superficialis (flexion at PIP): ALL median
- Interossei (dorsal abduct fingers; palmar adduct fingers): ALL ulnar
- Median does pronators
- Thumb: lots happening see next tweet!
18/
THUMB Radial, median, ulnar all participate!
Extension (thumbs up): RADIAL (the BEST, so thumbs up!)
Abduction (thumb out (90 degrees from palm)) MEDIAN
Adduction: thumb to index: ULNAR (just like other finger adduction: all ulnar)
Opposition: thumb to pinky MEDIAN
see fig
Extension (thumbs up): RADIAL (the BEST, so thumbs up!)
Abduction (thumb out (90 degrees from palm)) MEDIAN
Adduction: thumb to index: ULNAR (just like other finger adduction: all ulnar)
Opposition: thumb to pinky MEDIAN
see fig

MEDIAN Neuropathy
Most commonly at the wrist= Carpal tunnel syndrome
- Only muscles innervated distal to wrist can be affected: Abductor pollicis brevis (thumb abduction) most common
- sensory = lateral hand (thumb side) splitting ring finger
20/
Most commonly at the wrist= Carpal tunnel syndrome
- Only muscles innervated distal to wrist can be affected: Abductor pollicis brevis (thumb abduction) most common
- sensory = lateral hand (thumb side) splitting ring finger
20/
MEDIAN neuropathy 2:
Very rarely compressed in forearm=finger flexors can be affected
Gourmet for neuro geeks:
Anterior interosseous branch (AIN) of median:
- Flexor pollicis longus
- FDP 1-2
- Pronator quadratus
(Parsonage-Turner likes this nerve and long thoracic)
21/
Very rarely compressed in forearm=finger flexors can be affected
Gourmet for neuro geeks:
Anterior interosseous branch (AIN) of median:
- Flexor pollicis longus
- FDP 1-2
- Pronator quadratus
(Parsonage-Turner likes this nerve and long thoracic)
21/
ULNAR neuropathy 1
Most commonly at ELBOW, affecting all of its muscles:
- most noticeable in finger abduction/adduction (interossei) and FDP 3-4
- note sensory territory of ulnar is only DISTAL to wrist. So even w/compression at elbow, sensory loss only distal to wrist
22
Most commonly at ELBOW, affecting all of its muscles:
- most noticeable in finger abduction/adduction (interossei) and FDP 3-4
- note sensory territory of ulnar is only DISTAL to wrist. So even w/compression at elbow, sensory loss only distal to wrist
22
...if it looks like ulnar neuropathy, but sensory loss in medial forearm, consider radiculopathy (C8) or plexopathy affecting medial antebrachial cutaneous (branch of medial cord)
23/
23/
ULNAR neuropathy 2
Rarely ulnar nerve can be compressed at wrist (Guyon canal): then can only affect intrinsic hand muscles: abduction/adduction, sparing finger flexors (innervated in arm)
24/
Rarely ulnar nerve can be compressed at wrist (Guyon canal): then can only affect intrinsic hand muscles: abduction/adduction, sparing finger flexors (innervated in arm)
24/
So in sum, some tables from amazon.com
Even though the brachial plexus is proximal anatomically, to me it's distal understanding-wise😀 so we'll do that next now that you understand its most clinically important terminal branches!
Even though the brachial plexus is proximal anatomically, to me it's distal understanding-wise😀 so we'll do that next now that you understand its most clinically important terminal branches!
جاري تحميل الاقتراحات...